Right Hemithyroidectomy
Abstract
Hemithyroidectomy, or unilateral thyroid lobectomy, refers to removal of half the thyroid gland. The procedure is typically performed for suspicious thyroid nodules or small differentiated thyroid cancers based on biopsy via fine needle aspiration (FNA) and occasionally for symptomatic benign thyroid nodules. At most institutions the operation can be completed safely in outpatient fashion with patient discharge from the hospital the same day. It is typically performed via a transcervical collar incision, but endoscopic and transoral routes have been described. The procedure involves mobilization of the thyroid lobe, ligation of thyroid vessels, preservation of parathyroids, protection of the recurrent laryngeal nerve and dissection away from the trachea. In this patient, a thyroid nodule was detected and found to have indeterminate features on biopsy via FNA. A hemithyroidectomy was then performed for diagnostic purposes.
Case Overview
Background
Thyroid nodules are a common clinical finding; nearly 20-70% of individuals who undergo cervical ultrasound may have thyroid nodules.1,2 Although the majority of these nodules are benign, 7-15% of patients may have a thyroid cancer3,4 of which more than 90% are differentiated (papillary or follicular cancers).5 Based on ultrasonographic characteristics, thyroid nodules can be classified as benign, low suspicion, intermediate suspicion or high suspicion for malignancy.6 Clinicians use ultrasonographic characteristics of the nodule as well as thyroid function laboratory studies to determine whether a nodule should be biopsied with fine needle aspiration (FNA). Once a radiologically suspicious nodule is biopsied, a cytopathologist categorizes the cells based on the Bethesda classification system, which provides endocrinologists and endocrine surgeons an estimate of the risk of malignancy.7,8 This information can then be used to determine which patients require a hemithyroidectomy or may benefit from molecular profiling.9
Focused History of Patient
The patient is a 51-year-old male who was incidentally found to have a right thyroid nodule on a CT scan of the chest which was obtained following a motor vehicle accident. He did not have any symptoms or signs of hyper- or hypothyroidism. He then presented to his primary care doctor who performed a physical exam, ordered thyroid function labs, imaging, and ultimately, an FNA biopsy. Laboratory studies were normal. Ultrasound revealed a 2.3 cm right thyroid lobe nodule with highly suspicious features. The biopsy was deemed to be consistent with “atypia of undetermined significance” or AUS. The patient also did have a family history of thyroid cancer; both his sister and paternal grandfather were treated for papillary thyroid carcinoma. Given his family history, ultrasonographic and biopsy findings, a diagnostic hemithyroidectomy was recommended.
Physical Exam
Evaluation of thyroid nodules begins with a physical exam focusing on the thyroid gland as well as adjacent cervical lymph nodes.6 The thyroid gland should be assessed for additional nodules. Additional nodules may ultimately influence the operation performed. The texture of the nodule and its mobility should be evaluated. Fixed, firm nodules may indicate a more aggressive pathology. Any lymphadenopathy or scars from previous neck operations should be noted. Lymphadenopathy may signify metastatic spread of a cancer. Abnormalities in the patient’s voice as noted by the patient, family members, or physician should be assessed further and may require laryngoscopy to rule out recurrent laryngeal nerve involvement. The patient’s body habitus, neck width, neck length, natural skin creases, and thyroid/nodule size assist the surgeon in deciding where the incision should be placed.
For this particular patient, there was an incidentally-discovered 2.3 cm nodule in the right thyroid lobe. He was a lean gentleman and thus, the nodule was palpable on physical exam. It was mobile and rubbery. There were no additional palpable nodules in the thyroid. There was no evidence of cervical lymphadenopathy, no voice changes, and no previous surgical scars. The patient’s BMI was 23 and he had a height-appropriate neck width and length. All usual landmarks including the borders of the sternocleidomastoid muscles, thyroid and cricoid cartilages, and suprasternal notch were easily discernible and palpable.
Imaging
Thyroid ultrasonography is the imaging modality of choice for patients with a suspected thyroid nodule or radiographic finding suggestive of a thyroid nodule seen incidentally on another imaging (CT scan, etc.).6 Ultrasound can help characterize the size of the nodule as well as obtain important data regarding nodule features. These features include composition, echogenicity, margins, presence of calcifications, and shape. Collectively, this information can then be used to risk stratify a nodule and determine whether FNA is indicated. In general, findings of hypoechogenicity, irregularity, nodules that are taller than wide, and presence of microcalcifications within the nodule increase the risk for a possible malignancy.6 Other imaging modalities such as CT scan or MRI of the neck are typically reserved for patients with more advanced disease such as aggressive carcinomas with local or extensive nodal extension.6
For this patient, ultrasound revealed a heterogenous nodule measuring 2.3 cm in greatest dimension with microcalcifications as shown in Figures 1 and 2.
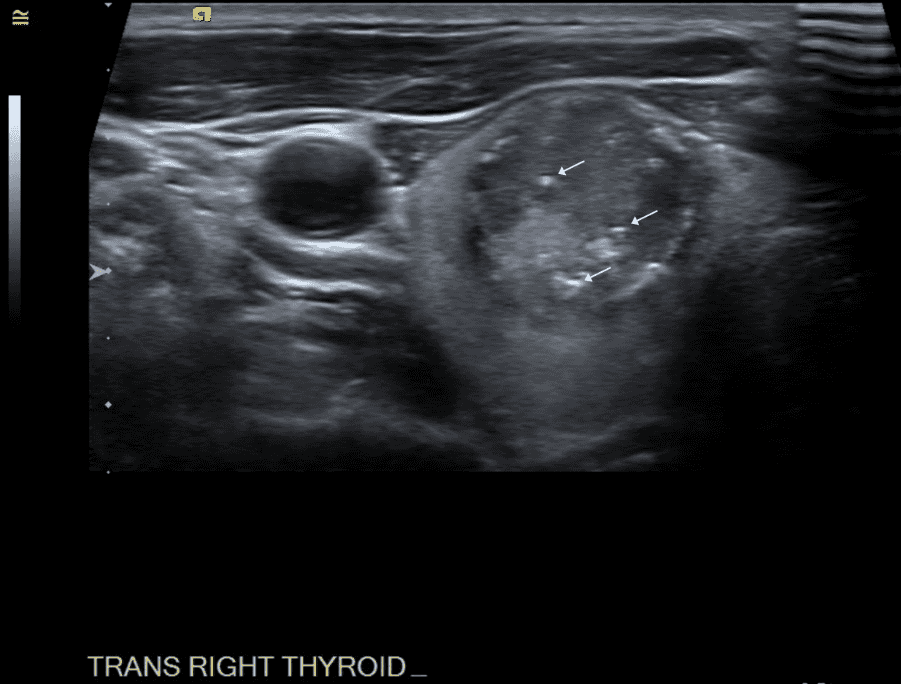 Figure 1. Transverse view of nodule within right thyroid lobe; white arrows denote microcalcifications.
Figure 1. Transverse view of nodule within right thyroid lobe; white arrows denote microcalcifications.
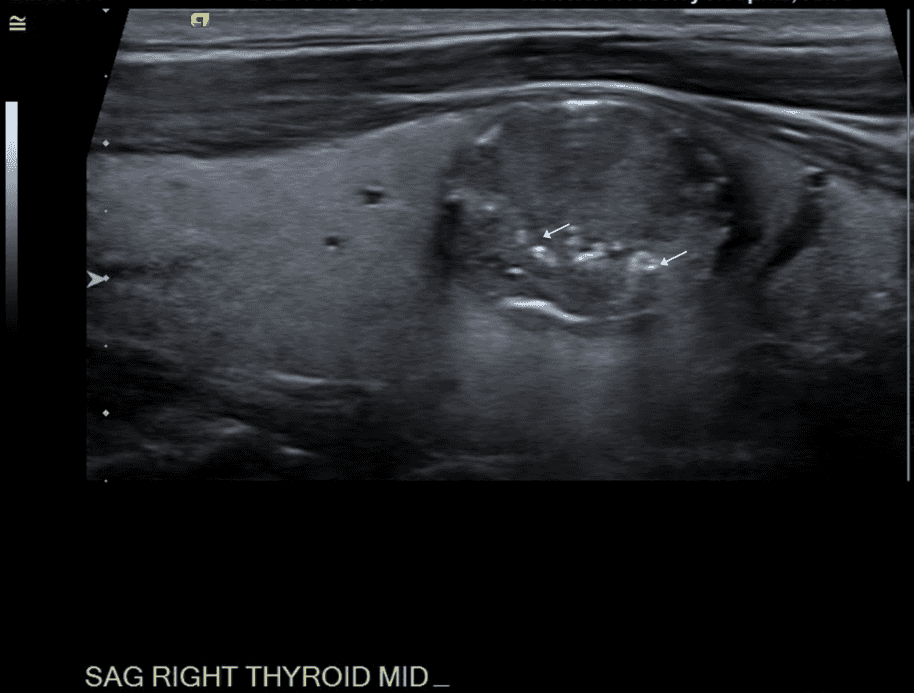 Figure 2. Sagittal view of nodule.
Figure 2. Sagittal view of nodule.
Natural History
The natural history of cytologically benign nodules is not fully understood; however, available data would suggest that a majority of nodules do increase in size in the subsequent 3-5 years after initial detection.10,11 Ultimately, this may require surgery due to symptoms or repeat biopsy. However, it does not appear that growth of a nodule correlates to an increased risk of malignancy.10-12
The natural history of untreated, biopsy-proven differentiated thyroid cancer is more difficult to understand, given that most of these patients undergo surgery. However, there has been recent interest in the observation of small papillary thyroid cancers less than 1 cm in size, as long as there are no risk factors for more advanced or aggressive disease. With limited data, it appears that these small papillary carcinomas do not progress dramatically over time and that many of them can be observed without treatment.13
Options for Treatment
Treatment options for thyroid nodules depend on radiographic findings, biopsy results, thyroid function studies, and local symptoms. If a nodule appears benign on ultrasound, is not causing symptoms, and is not causing hyperthyroidism, it may be observed. Benign-appearing nodules that are consistent with a toxic adenoma or toxic multinodular goiter may be treated with surgery, radioiodine therapy, or thionamides. Sonographically suspicious nodules should be biopsied. If biopsy results are benign, observation can be pursued. Repeat biopsy may be indicated if the initial FNA is nondiagnostic. For patients with indeterminate or suspicious biopsy results, further risk stratification can be obtained with molecular profiling tests, or patients may consider undergoing a diagnostic hemithyroidectomy.6 Observation is also an option, depending on patient risk factors. For those with indeterminate/suspicious biopsy results and several nodules in the bilateral thyroid lobes or with underlying hypothyroidism, a total thyroidectomy could be considered as an initial treatment.
Rationale for Treatment
This patient has several reasons to proceed with surgery, and specifically a diagnostic hemithyroidectomy. First, the nodule had suspicious features based on ultrasound. Second, the biopsy results were indeterminate. Third, he has a family history of thyroid cancer, which increases his overall risk. He could have considered molecular profiling of the nodule, to further risk stratify his lesion if he truly wanted to avoid surgery. However, given that he is otherwise fit and healthy, a low-risk procedure such as a hemithyroidectomy is a very reasonable and definitive route to pursue compared with molecular profiling.
Discussion
The history of thyroid surgery dates back to the 1800s when Theodor Billroth began performing the operation in Switzerland. At that time, outcomes were poor and therefore several of his surgical assistants and trainees attempted to improve them. Most successful was Theodor Kocher, who first described unilateral lobectomy in an attempt to minimize postoperative hypothyroidism.14
Since that era, thyroidectomy has become a very safe operation with very low rates of complications. In many centers, a hemithyroidectomy is completed in an outpatient fashion. Patients are typically discharged home within a few hours after surgery.
Historically, thyroid cancer was treated aggressively, with most patients undergoing total thyroidectomy. Current literature would suggest that there is little to no difference in survival among select patients with small, low-risk cancers who undergo hemithyroidectomy vs. total thyroidectomy.6,15 Thus, more patients are being given the option of a hemithyroidectomy, especially in the case of an indeterminate or suspicious nodule based on biopsy. In addition, a significant amount of research is being conducted on the genetic and molecular basis of thyroid cancer, which may lead to the creation of genetic targets for treatment. Collectively, these findings may lead to the need for less aggressive thyroid surgery in the future. Ultimately, the decision for surgery the extent of the operation is a discussion between the surgeon, endocrinologists, and the patient.
For this patient, final pathology revealed a papillary thyroid carcinoma measuring 2.1 cm in maximum dimension. There were no other features to suggest aggressive disease; however, the patient carefully considered the risks and benefits of contralateral lobe observation vs. completion thyroidectomy. Given his family history, he ultimately elected to proceed with completion thyroidectomy, which was performed without complication. He is now doing well with ongoing surveillance.
Equipment
Nerveana nerve locator, Neurovision Medical Products
Disclosures
The authors have no disclosures to report.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997;126(3):226-231. doi:10.7326/0003-4819-126-3-199702010-00009.
- Guth S, Theune U, Aberle J, Galach A, Bamberger CM. Very high prevalence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest. 2009;39(8):699-706. doi:10.1111/j.1365-2362.2009.02162.x.
- Hegedüs L. The thyroid nodule. N Engl J Med. 2004;351(17):1764-1771. doi:10.1056/NEJMcp031436.
- Mandel SJ. A 64-year-old woman with a thyroid nodule. JAMA. 2004;292(21):2632-2642. doi:10.1001/jama.292.21.2632.
- Sherman SI. Thyroid carcinoma. Lancet. 2003;361(9356):501-511. doi:10.1016/S0140-6736(03)12488-9.
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133. doi:10.1089/thy.2015.0020.
- Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol. 2009;132(5):658-665. doi:10.1309/AJCPPHLWMI3JV4LA.
- Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L, Baloch ZW. The Bethesda System for Reporting Thyroid Cytopathology: a meta-analysis. Acta Cytol. 2012;56(4):333-339. doi:10.1159/000339959.
- Ferris RL, Baloch Z, Bernet V, et al; American Thyroid Association Surgical Affairs Committee. American Thyroid Association Statement on Surgical Application of Molecular Profiling for Thyroid Nodules: Current Impact on Perioperative Decision Making. Thyroid. 2015;25(7):760-768. doi:10.1089/thy.2014.0502.
- Alexander EK, Hurwitz S, Heering JP, et al. Natural history of benign solid and cystic thyroid nodules. Ann Intern Med. 2003;138(4):315-318. doi:10.7326/0003-4819-138-4-200302180-00010.
- Ajmal S, Rapoport S, Ramirez Batlle H, Mazzaglia PJ. The natural history of the benign thyroid nodule: what is the appropriate follow-up strategy? J Am Coll Surg. 2015;220(6):987-992. doi:10.1016/j.jamcollsurg.2014.12.010.
- Durante C, Costante G, Lucisano G, et al. The natural history of benign thyroid nodules. JAMA. 2015;313(9):926-935. doi:10.1001/jama.2015.0956.
- Miyauchi A. Clinical Trials of Active Surveillance of Papillary Microcarcinoma of the Thyroid. World J Surg. 2016;40(3):516-522. doi:10.1007/s00268-015-3392-y.
- Hannan SA. The magnificent seven: a history of modern thyroid surgery. Int J Surg. 2006;4(3):187-191. doi:10.1016/j.ijsu.2006.03.002.
- Welch HG, Doherty GM. Saving thyroids – overtreatment of small papillary cancers. N Engl J Med. 2018;379(4):310-312. doi:10.1056/NEJMp1804426.


| Publication Date | N/A |
| Article ID | 21 |
| Production ID | 0096 |
| Volume | N/A |
| Issue | 21 |
| DOI | |
| https://doi.org/10.24296/jomi/21 | |