Site-Specific Posterior Colporrhaphy and Perineorrhaphy for Rectocele
Abstract
The patient is a 38-year-old female who presented with fecal incontinence, constipation, and stress urinary incontinence. She was found to have stage II posterior vaginal wall prolapse. She desired definitive surgical management of her prolapse and opted for posterior vaginal repair. Although stress urinary incontinence was demonstrated on urodynamic testing, the decision was made not to proceed with concurrent midurethral sling given her history of pelvic floor dyssynergia and intermittent urinary retention. The surgery was uncomplicated, and she was discharged on the day of surgery. Her recovery was unremarkable.
Case Overview
Background
The patient is a 38-year-old G3P3 female with a history of celiac disease who presented to the urogynecology office with fecal incontinence, constipation, and stress urinary incontinence. She has a history of three vaginal deliveries, one of which was forceps-assisted. Her largest baby was 7 pounds 14 ounces.
The patient reported long-standing constipation since childhood that had worsened since her diagnosis of celiac disease. She was followed by the colorectal surgery service and was found to have a nonrelaxing puborectalis on electromyography (EMG), consistent with pelvic floor dyssynergia. She admitted to straining and vaginal splinting during defecation. She was started on a bowel regimen and was referred to pelvic physical therapy, which helped to decrease the straining. She also had symptoms of stress urinary incontinence that improved with pelvic floor physical therapy.
Physical Examination
Her physical examination was consistent with stage II anterior and posterior vaginal wall prolapse. The posterior vaginal wall was at the hymen, and there was demonstrable rectovaginal pocketing. The anterior vaginal wall was 1 cm above the hymen. Apical support and total vaginal length were normal. The perineal body was normal; however, the genital hiatus was enlarged at 5 cm. See Figure 1 for a graphic demonstration of preoperative prolapse.
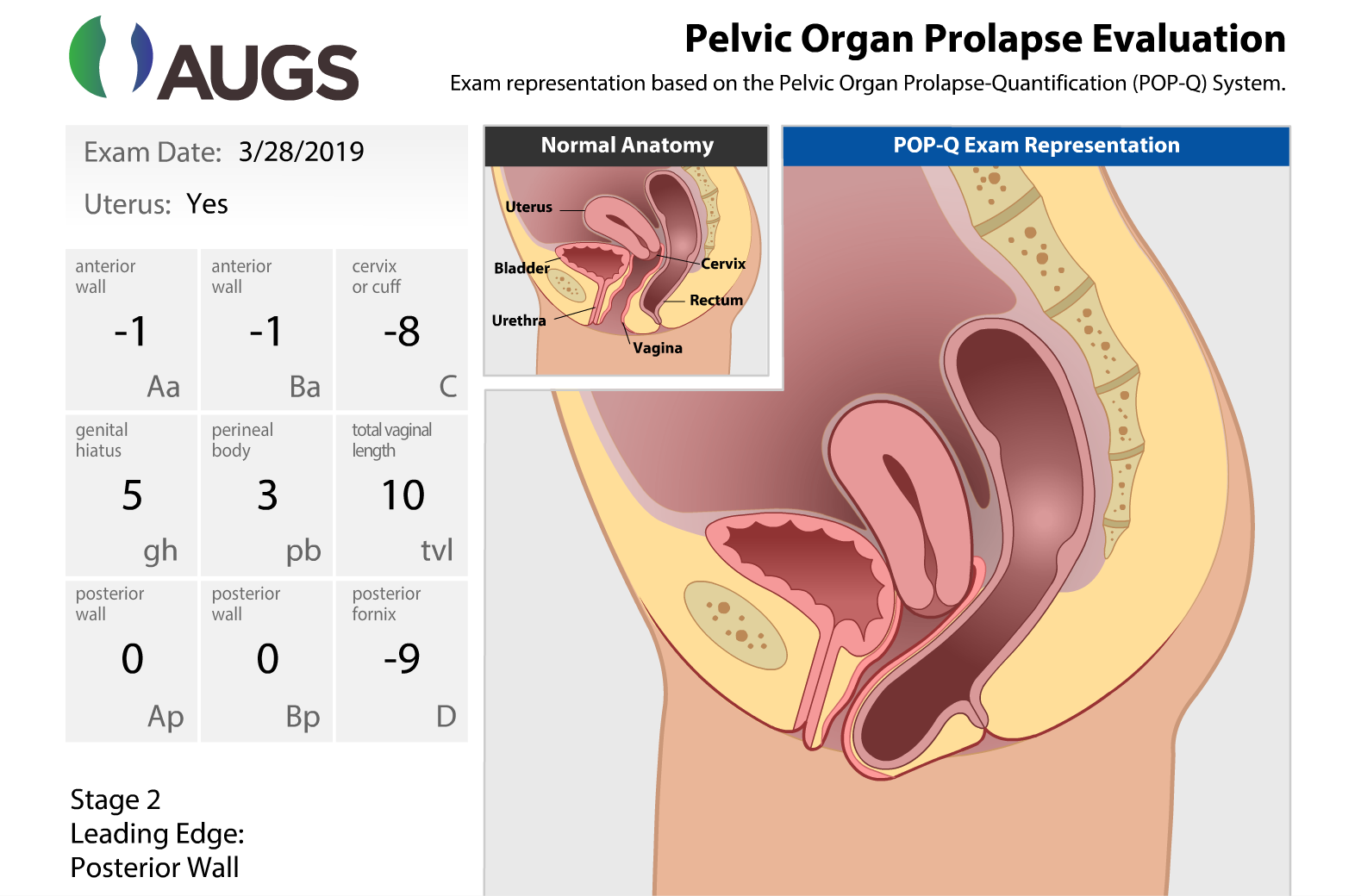
Figure 1. POP-Q Measurements
A graphic demonstration of preoperative POP-Q measurements.
Used with permission from the American Urogynecologic Society (AUGS).
Imaging
Due to an elevated post-void residual, the patient underwent a renal ultrasound, thus ruling out hydronephrosis.
Other Testing
She had urodynamic testing that showed stress urinary incontinence at a low volume, urgency urinary incontinence, and incomplete voiding.
Options for Treatment
Treatment of vaginal prolapse depends on the individual patient’s symptoms and goals. Options include expectant management, pelvic floor exercises, pelvic floor physical therapy, pessary, and surgical management (Figure 2). Because the patient found the prolapse bothersome, she declined expectant management and preferred to move forward with definitive surgical management.
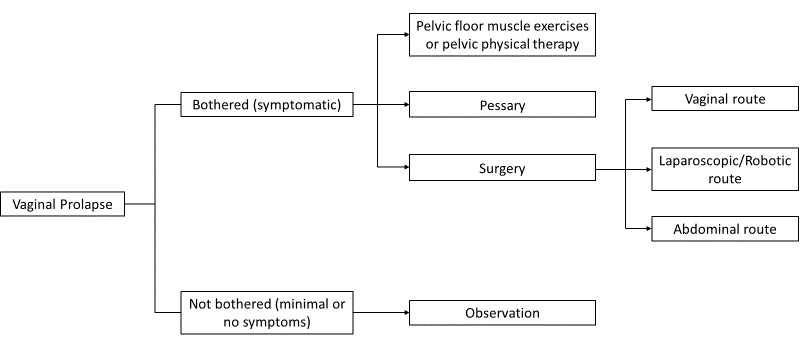
Figure 2. Prolapse Decision Tree
A flow chart representation of the prolapse decision tree.
Rationale for Treatment
The patient decided that she wanted a reconstructive surgery that was minimally invasive and and that would involve only her own tissues (i.e., no mesh).
Special Considerations
As described above, the patient underwent urodynamic testing, which is most often performed preoperatively to assess for possible occult stress urinary incontinence, which is urinary incontinence that is “unmasked” by the prolapse repair. During the testing, the prolapse is elevated to simulate the repair and the patient is taken through various maneuvers to elicit stress urinary incontinence. If the patient has urinary leakage during testing, she has a 58% chance of having urinary incontinence after the prolapse repair.1 There is a 38% chance that the patient may have leaking, even if the testing is negative, and may require a separate staged procedure to address the incontinence.1
Given the presence of pelvic floor dyssynergia on prior testing, presence of significant detrusor overactivity, and the improvement of stress urinary incontinence with pelvic floor physical therapy, the patient was advised not to proceed with concomitant midurethral sling at the time of prolapse repair. The patient agreed with the plan and understood that she may experience worsening urinary incontinence postoperatively.
Posterior vaginal wall prolapse can be addressed in several ways. Traditional native-tissue posterior colporrhaphy involves a midline plication of the rectovaginal muscularis, whereas a site-specific defect repair aims to reapproximate the broken edges of the fibromuscularis and correct all defects. Alternatively, posterior colporrhaphy can be performed with biologic graft augmentation. Traditional native-tissue posterior colporrhaphy and site-specific defect repairs have similar anatomic and functional outcomes.2 A biologic graft does not improve the anatomic outcome in the posterior wall, and one study actually showed an increased anatomic failure rate with porcine-biologic graft augmentation in comparison to traditional or site-specific posterior colporrhaphies.2
Our clinical practice is to address any specific defects found at the time of posterior colporrhaphy.
Discussion
The patient was taken to the operating room where general anesthesia was given, and a laryngeal mask airway was obtained. Sequential compression devices were placed on the lower extremities as venous thromboembolism prophylaxis and intravenous cefazolin was given as antibiotic prophylaxis. She was placed in the dorsal lithotomy position in candy cane stirrups. A timeout was performed with the entire operative staff. A Foley catheter was placed to drain the bladder.
The anterior vaginal wall revision was performed first. The area of anticipated dissection was injected with dilute 0.25% Marcaine with epinephrine. A transverse incision was then made at the level of the vaginal wall lappets, approximately 3 cm proximal to the urethra. The vaginal epithelium was then sparingly dissected off of the underlying pubocervical connective tissue and trimmed to remove the redundant vagina. The incision was then closed in a transverse manner with a running 2-0 Vicryl suture.
The posterior repair was performed next. A dilute solution of Marcaine with epinephrine was injected under the perineal skin and the posterior vaginal wall. The attenuated scarred perineal skin was excised. The posterior vaginal wall was dissected sharply off of the underlying rectum. The rectocele was then closed in a site-specific fashion; first, it was noted that the proximal edge and both lateral edges of the rectovaginal fascia had been detached. All sites were reattached with a running 2-0 PDS suture. Irrigation was performed, and excellent hemostasis was noted. Excess posterior vaginal wall was excised. The incision was closed with 2-0 Vicryl in a running stitch down to 3 cm above the hymen and held. Interrupted stitches of 0 Vicryl were placed to build up the perineal body and decrease the genital hiatus. The midline incision was then closed in a running fashion using 2-0 Vicryl suture. The perineum was closed with submucosal and subcutaneous interrupted stitches. A final rectal exam was performed, confirming that there were no stitches in the rectum and that there was good support to the anterior rectal wall and the perineal body. The vagina was irrigated, and hemostasis ensured. The Foley catheter was removed, and the procedure was deemed complete.
Postoperative Course
Approximately two hours after surgery, the patient underwent a backfill trial of void. The bladder was backfilled via the Foley catheter with 300 ml of sterile water. The Foley catheter was removed, and the patient was able to void more than 200 ml, thereby passing the trial of void. Subsequently, because she met all discharge criteria, she went home on the day of surgery.
The patient was seen two weeks after surgery. She was doing well and denied any vaginal bulge or voiding dysfunction.
Equipment
Cystoscopy equipment with 70-degree lens in order to visualize ureteral jets.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Visco AG, Brubaker L, Nygaard I, et al.; Pelvic Floor Disorders Network. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607-614. doi:10.1007/s00192-007-0498-2.
- Paraiso MF, Barber MD, Muir TW, Walters MD. Rectocele repair: a randomized trial of three surgical techniques including graft augmentation. Am J Obstet Gynecol. 2006;195(6):1762-1771. doi:10.1016/j.ajog.2006.07.026.


| Publication Date | 6/15/2022 |
| Article ID | 269 |
| Production ID | 0269 |
| Volume | 2022 |
| Issue | 269 |
| DOI | |
| https://doi.org/10.24296/jomi/269 | |