Deltoid Ligament Repair
Abstract
Injury to the medial deltoid ligament complex is rare as it is the strongest of the ankle ligaments. However, damage to this structure can occur, often in association with an avulsion fracture of the medial malleolus due to the ligamentous strength of the complex. Deltoid ligament repair remains a primary option for patients with severe acute injuries, or patients with chronic instability who have failed conservative measures. Repair of the medial ankle ligaments provides improved stability with reduced risk of recurrent sprains and potential damage to local cartilage. We present a case of a young woman with concomitant medial and lateral ankle instability who successfully underwent deltoid ligament repair for her medial ligament injury.
Keywords
Ankle sprain; medial ligament complex; deltoid ligament repair; ankle instability.
Case Overview
Background
Injury to the medial deltoid ligaments is rare as collectively this complex is the strongest of the ankle ligaments.1 However, damage to this structure can occur, often in association with an avulsion fracture of the medial malleolus due to the ligamentous strength of the complex.11 The deltoid ligament is comprised of the medial collateral ligaments of the ankle, with a superficial layer that includes the tibionavicular, tibiospring, tibiocalcaneal, and superficial posterior tibiotalar ligaments, as well as a deep layer that includes the anterior tibiotalar and deep posterior tibiotalar ligaments.2 Diagnosis and management of medial ankle instability remain challenging and are rarely discussed in the literature. We present a case of medial ankle instability due to injury to the deltoid ligament managed successfully by open repair.
Focused History of the Patient
This patient presented with medial ankle pain and reported instability in association with concomitant lateral ankle instability. Typically, patients report the onset of symptoms following an acute traumatic eversion event, with inability to bear weight.3 Patients may also present with a more chronic injury to the medial ankle region, with the ankle described as “giving way” or loose, particularly on uneven ground. Pain may be reported, and often radiates laterally due to subfibular impingement from associated hindfoot valgus.
In assessment of ankle injuries, obtaining information such as the nature of the injury, whether the patient could weight bear following the injury, and whether prior injury has occurred is critical to the history for treatment planning purposes.3
Physical Exam
Physical examination of patients with suspected medial ankle instability should begin with bilateral inspection of the ankles in standing, walking, and sitting position.3, 4 The examiner should note any swelling, hematoma, malalignment, deformity, or scars, as well as asymmetrical planovalgus and abductus upon weight-bearing. Inspection should be followed by palpation of the medial and lateral ligaments and joint spaces in addition to the syndesmosis and posterior tibial, peroneal, and Achilles tendons. Tenderness in the medial gutter overlying the deltoid ligament is commonly seen with injury. Tenderness along the posterior tibial tendon may indicate associated posterior tibial tendon insufficiency, which often co-occurs. Eversion and external rotation stress tests can assess stability of the deep and superficial deltoid ligaments, and the anterior drawer test may be used to diagnose anteromedial subluxation.
Imaging
For acute injuries, standard radiographs should be obtained to exclude concurrent widening of the medial ankle clear space, deltoid avulsion fragments, syndesmotic injuries, and ankle fractures.3, 4 MRI and ultrasound play an important adjunct role to be used when acute or chronic injury is suspected. Preoperative MRI can help elucidate associated pathology and provide valuable insight into operative planning; however, up to 20% of patients will have false negative results on MRI when evaluating acute deltoid ligament complex injury.5 Ultrasound has been shown to be useful particularly in acute ligamentous ankle injuries, with a sensitivity of 94% and specificity of 100% in detecting anterior talofibular ligament tears against MRI.6–8
Natural History
Isolated acute medial ankle instability as a result of minor deltoid ligament injury may be managed conservatively and some patients may become asymptomatic depending on the severity of the tear. However, patients remain at risk for progression to chronic medial ankle instability, injury recurrence, and long-term complications such as osteoarthritis.3 Severe ankle injury is unlikely to improve without intervention, with a greater risk of these complications.
Options for Treatment
Conservative management with protection, rest, ice, compression, and elevation may be attempted for minor isolated acute injuries for 1–2 weeks. A soft ankle orthosis may be added for Grade I sprains, though Grade II–III sprains may require a stronger brace or walker to prevent eversion for up to 6 weeks. Physiotherapy protocols should be included as early as possible to maximize range of motion and strength.
Isolated acute Grade II–III sprains may require operative intervention if evaluation reveals additional injuries or the patient participates in high-level athletics. Arthroscopy should be employed to confirm diagnosis before further surgical intervention such as deltoid ligament repair.
Chronic medial ankle instability may be treated with similar conservative measures for 3–6 months, at which time patients may be considered for operative intervention including deltoid ligament repair if they fail to become asymptomatic, or if associated pathology warrants earlier intervention. Patients with limitations in their daily activities, recurrent sprains, or worsening deformities are indicated for surgical intervention.
Rationale for Treatment
Surgical intervention with deltoid ligament repair can significantly improve stabilization of the medial ankle ligament complex and prevent progression to chronic instability.3 Goals of surgery also include the correction of deformities such as hindfoot valgus or pes planovalgus et abductus, and prevention of future sprains and potential damage to the cartilage. Common associated injuries are addressed on a case-by-case basis depending on the type and severity of co-injury.
Discussion
The patient successfully underwent deltoid ligament repair. An incision was made over the medial gutter of the ankle, and dissection was carried down to the anterior fibers of the deltoid ligament. The saphenous nerve and vein were protected. An avulsion of the anterior fibers of the deltoid ligament off of the anterior aspect of the medial malleolus was noted. Laxity of the incompetent ligament was observed upon testing for range of motion intraoperatively. A rasp was used to prepare the bone prior to drilling, and the resulting debris was irrigated out of the wound. Drill holes were made proximally, and a suture anchor was placed. The sutures were then passed through the proximal portion of the anterior fibers of the deltoid ligament, and these were tied down to their origin. The ankle was put through a range of motion to test for stability and ensure that the repair remained intact under stress. The wound was then thoroughly irrigated and closed in a layered fashion.
Conservative measures have been shown to be helpful for patients with minor medial ankle injuries. Physiotherapy programs may improve range of motion and muscular strength leading to better stabilization, and these measures are typically incorporated as soon as the patient is able following an acute injury. For more severe injuries including Grade II–III ankle sprains, operative intervention may be required in the setting of additional injury, including fractures, dislocation, and injuries to the syndesmosis.3
Of note, ankle arthroscopy should be performed prior to deltoid ligament repair to confirm the diagnosis, assess the degree of insufficiency, and to exclude additional pathology.9 More recently, a new treatment strategy involving augmentation of the repaired ligament construct with an internal brace has been employed.10 Patients undergoing this procedure were shown to have significantly improved FAAM and SF-36 scores with no evidence tradeoff in terms of stability or reoperation. While further study is needed, this may be of benefit to future patients with chronic medial ankle instability.
Although the arthroscopic evaluation for this case was not filmed, Figure 1 represents a similar case of the avulsion of medial fibers of the superficial deltoid ligament.17
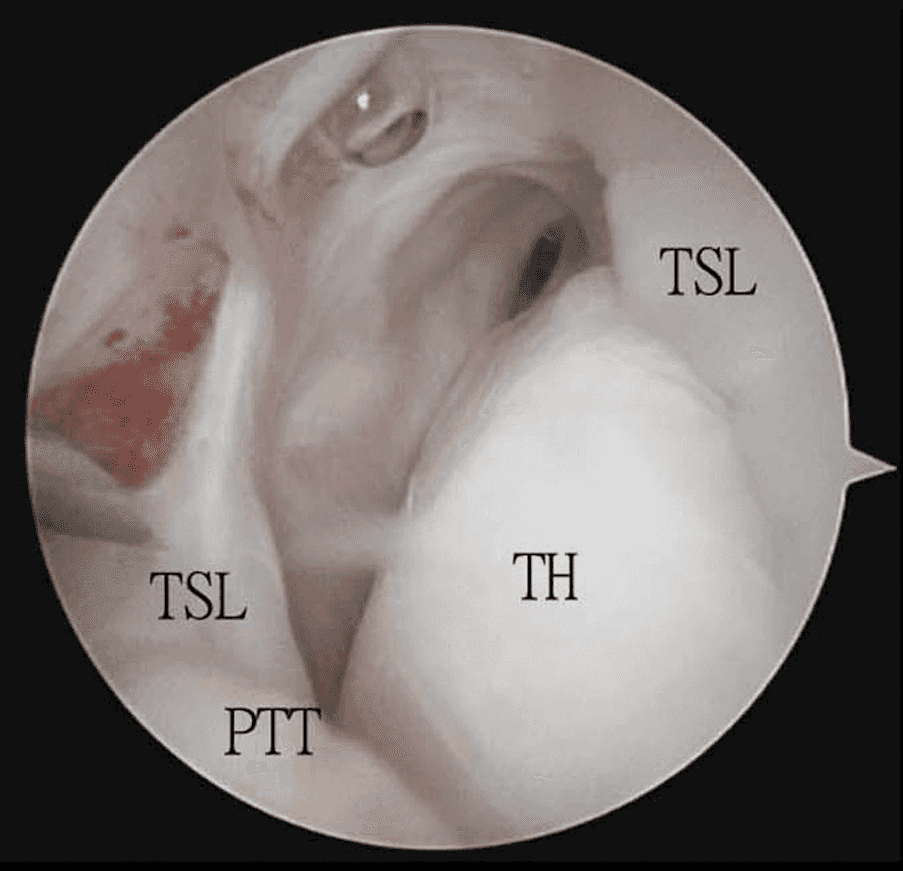
Figure 1. The arthroscopic view shows avulsion of the tibio-spring ligament (TSL), and the exposed talar head (TH). The posterior tibial tendon (PTT) is retracted in a plantar direction.
Some degree of controversy exists surrounding the need to perform deltoid ligament repair in the context of a malleolar fracture. Yu et al. reported 131 patients with ankle fractures and noted a significant improvement in AOFAS ankle-hindfoot scores, visual analog scale (VAS) scores, and Medical Outcomes Study Short Form 36-item questionnaire scores compared to preoperative status.5 However, several studies are questioning the necessity of repairing the deltoid ligament if a successful open reduction and internal fixation (ORIF) was performed.11–13 Patients described “satisfactory” outcomes when ORIF was performed without deltoid ligament repair. Of note, these studies did report a significant finding of residual ankle pain in long-term follow up, so further study is warranted.
Deltoid ligament reconstruction may also be performed in the setting of valgus ankle osteoarthritis when a corrective osseous procedure is also planned.14,15 Due to the nature of longstanding osseous abnormalities associated with the pathogenesis of osteoarthritis, isolated deltoid ligament repair is unlikely to be effective as a treatment option, but may be used as an adjunct to a corrective osseous procedure as described by Pagenstert.16
Equipment
- Depuy Mitek Suture Anchor
- Rasp
- Self-stopping drill guide
- Surgical drill
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Additional Information
This article is the companion to the following JOMI articles by Dr. Eric Bluman, MD, PhD:
Citations
- Butler AM, Walsh WR. Mechanical response of ankle ligaments at low loads. Foot Ankle Int. 2004 Jan;25(1):8-12. doi:10.1177/107110070402500103.
- Hintermann B, Golanó P. The anatomy and function of the deltoid ligament. Tech Foot Ankle Surg. 2014;13(2):67-72. doi:10.1097/BTF.0000000000000044.
- Alshalawi S, Galhoum AE, Alrashidi Y, et al. Medial ankle instability: the deltoid dilemma. Foot Ankle Clin. 2018;23(4):639-657. doi:10.1016/j.fcl.2018.07.008.
- Corte-Real N, Caetano J. Ankle and syndesmosis instability: consensus and controversies. EFORT Open Rev. 2021 Jun 28;6(6):420-431. doi:10.1302/2058-5241.6.210017.
- Yu GR, Zhang MZ, Aiyer A, et al. Repair of the acute deltoid ligament complex rupture associated with ankle fractures: a multicenter clinical study. J Foot Ankle Surg. 2015;54(2):198-202. doi:10.1053/j.jfas.2014.12.013.
- Henari S, Banks LN, Radiovanovic I, Queally J, Morris S. Ultrasonography as a diagnostic tool in assessing deltoid ligament injury in supination external rotation fractures of the ankle. Orthopedics. 2011;34(10). doi:10.3928/01477447-20110826-11.
- Allison SJ, Nazarian LN. Musculoskeletal ultrasound: evaluation of ankle tendons and ligaments. AJR Am J Roentgenol. 2010;194(6). doi:10.2214/AJR.09.4067.
- Sconfienza LM, Orlandi D, Lacelli F, Serafini G, Silvestri E. Dynamic high-resolution US of ankle and midfoot ligaments: normal anatomic structure and imaging technique. Radiographics. 2015 Jan-Feb;35(1):164-78. doi:10.1148/rg.351130139.
- Arthur D, Pyle C, Shymon SJ, Lee D, Harris T. Correlating arthroscopic and radiographic findings of deep deltoid ligament injuries in rotational ankle fractures. Foot Ankle Int. 2020;42(3). doi:10.1177/1071100720962796.
- Pellegrini MJ, Torres N, Cuchacovich NR, Huertas P, Muñoz G, Carcuro GM. Chronic deltoid ligament insufficiency repair with Internal BraceTM augmentation. Foot Ankle Surg. 2019;25(6):812-818. doi:10.1016/j.fas.2018.10.004.
- Lee S, Lin J, Hamid KS, Bohl DD. Deltoid ligament rupture in ankle fracture: diagnosis and management. J Am Acad Orthop Surg. 2019 Jul 15;27(14):e648-e658. doi:10.5435/JAAOS-D-18-00198.
- Dabash S, Elabd A, Potter E, et al. Adding deltoid ligament repair in ankle fracture treatment: Is it necessary? A systematic review. Foot Ankle Surg. 2019 Dec;25(6):714-720. doi:10.1016/j.fas.2018.11.001.
- Hunt KJ, Phisitkul P, Pirolo J, Amendola A. High ankle sprains and syndesmotic injuries in athletes. J Am Acad Orthop Surg. 2015 Nov;23(11):661-73. doi:10.5435/JAAOS-D-13-00135.
- Hogan MC V, Dare DM, Deland JT. Is deltoid and lateral ligament reconstruction necessary in varus and valgus ankle osteoarthritis, and how should these procedures be performed? Foot Ankle Clin. 2013;18(3):517-527. doi:10.1016/j.fcl.2013.06.012.
- Savage-Elliott I, Murawski CD, Smyth NA, Golanó P, Kennedy JG. The deltoid ligament: an in-depth review of anatomy, function, and treatment strategies. Knee Surg Sport Traumatol Arthrosc. 2013;21(6):1316-1327. doi:10.1007/s00167-012-2159-3.
- Pagenstert GI, Hintermann B, Barg A, Leumann A, Valderrabano V. Realignment surgery as alternative treatment of varus and valgus ankle osteoarthritis. Clin Orthop Relat Res. 2007;462(462):156-168. doi:10.1097/BLO.0b013e318124a462.
- Lui TH. Endoscopic repair of the superficial deltoid ligament and spring ligament. Arthrosc Tech. 2016 Jun 13;5(3):e621-5. doi:10.1016/j.eats.2016.02.004.


| Publication Date | 7/18/2024 |
| Article ID | 91 |
| Production ID | 0091 |
| Volume | 2024 |
| Issue | 91 |
| DOI | |
| https://doi.org/10.24296/jomi/91 | |