Total Knee Arthroplasty
Abstract
Total knee replacement is one of the most common orthopaedic procedures performed in the United States. The most common indication for total knee replacement is osteoarthritis. Clinical signs of knee osteoarthritis include pain with walking, difficulty ranging the knee, knee instability, varus deformity, bony enlargement, extension lag, and flexion contracture. Radiologic evidence for osteoarthritis of the knee includes the presence of osteophytes, joint space narrowing, subchondral sclerosis, subchondral cysts, and malalignment.
Before considering total knee replacement, patients typically undergo a trial of less invasive treatments, including lifestyle modification, pharmacologic therapy, and injections. If these methods fail to produce satisfactory improvement in the patient’s symptoms, one should consider the benefits and risks of total knee replacement in conjunction with their surgeon. Outcomes following total knee replacement are excellent, with patients reporting greatly reduced pain, improved mobility, and improved quality of life. However, patients must be aware that there are serious risks that accompany any surgery, which include infection, pulmonary embolism, deep vein thrombosis, nerve damage, and need for further procedures.
Case Overview
Focused History
The patient is a 66-year-old female with bilateral knee pain, worse on the left. She has tried conservative treatment for several years including activity modification and oral analgesics without significant effect. Significant past surgical history includes two arthroscopic procedures to bilateral knees within the past seven years.
Tips for History
Some questions to ask:1,2
- How much pain do you have with walking? At rest? At night in bed?
- How many standard blocks/consecutive minutes can you walk for?
- Can you walk up stairs? With assistance?
- Do you hear clicking with motion?
- What is your knee range of motion?
- Does your knee feel unstable? Does your knee ever buckle with use?
- What assistive devices do you use?
- Do you have stiffness in the morning? Does it improve during the day?
While gathering past medical history, investigate risk factors for infection and other complications, such as rheumatoid arthritis, diabetes mellitus, poor nutritional status, obesity, concurrent urinary tract infection, steroid therapy, malignancy, hypokalemia, allogeneic blood transfusion, history of smoking, prior joint surgery and preoperative infection of teeth, skin or urinary tract, venous insufficiency.2
Physical Exam
On examination the patient is well appearing, resting comfortably in no acute distress. Distal neurovascular examination of the bilateral lower extremities demonstrates intact EHL and FHL function. Sensation is intact to light touch in the L4–S1 distribution. The bilateral knees have a range of motion from full extension to approximately 125 degrees of flexion. The knees are stable to varus and valgus stress as well as anterior and posterior drawer test. She has some effusion of the left knee. She has pain with walking and ambulates with an antalgic gait.
Tips for physical exam:1,2
- Visually inspect the knee. Assess for bony enlargement.
- Assess for joint effusion, redness, warmth, and bony tenderness.
- Assess joint line tenderness. Perform meniscal provocative maneuvers (McMurray’s and grind tests).
- Assess pain with hip flexion and range of motion to rule out hip as pain generator.
- Assess knee range of motion.
- Determine extension lag.
- Assess flexion contracture.
- Test medial and lateral stability of the knee.
- Test anterior and posterior stability of the knee.
- Determine alignment of the knee.
- Test lower extremity sensation at the foot in saphenous, sural, superficial peroneal, deep peroneal, and tibial distributions.
- Test lower extremity motor function with hip flexion, knee extension, ankle dorsiflexion, ankle plantarflexion, big toe flexion, and big toe extension.
- Assess femoral, popliteal, posterior tibial, and dorsalis pedis pulses.
- Observe patient’s gait. Assess for limp, need for assistance with standing and sitting.
Imaging
AP weight-bearing views including bilateral knees, lateral, and sunrise views are necessary to assess knee osteoarthritis radiographically. The critical findings of knee osteoarthritis on radiologic exam are as follows:2
- Joint space narrowing
- Osteophytes
- Subchondral sclerosis
- Subchondral cysts
- Loss of bone stock
- Malalignment
- Varus or valgus deformity
Finding osteophytes on x-ray best differentiates osteoarthritis from rheumatoid and other arthritides. A sensitive and specific criteria for knee osteoarthritis is the combination of knee pain, radiologic appearance of osteophytes and one or more of the following: age over 50 years, morning stiffness less than 30 minutes, or crepitus on active motion.
Bilateral weight-bearing views should be used to compare the affected with the unaffected side. Osteoarthritis should be assessed in each of the three knee compartments: medial, lateral, and patellofemoral. It should be noted that as many as 30% of adults over 65 years will demonstrate radiographic appearance of osteoarthritis, but one-third of these individuals will be asymptomatic.3 Thus, it is important to correlate clinical and radiographic findings to reach a diagnosis of symptomatic knee osteoarthritis, a clinically relevant entity.
Natural History
Among elderly patients, radiographic findings of osteoarthritis occur with an incidence of about 2% per year and symptomatic osteoarthritis occurs with an incidence of about 1% per year. Among individuals with radiographically evident findings of osteoarthritis, disease progression occurs at an incidence of about 4% per year. In each category, incidence of osteoarthritis is higher in women than in men.4
Options for Treatment
Treatment for osteoarthritis of the knee typically proceeds along a spectrum from least to most invasive. Initial management for symptomatic knee osteoarthritis should begin with a trial of education and lifestyle intervention in conjunction with pharmacologic treatment for an adequate period of time before proceeding to invasive therapies. Treatment should be tailored to patient-specific risk factors, patient’s level of pain and disability, inflammatory signs, and degree of structural damage. Treatment options are summarized below:3
- Non-pharmacologic treatments. These include education, exercise, physical therapy, weight loss, insoles, bracing, and lifestyle changes.
- Pharmacologic treatments. These include paracetamol, NSAIDs, opioids, topical treatments, glucosamine, and chondroitin. Paracetamol is the best initial oral medication and preferred long-term if effective. If no response is observed with paracetamol, treatment with NSAIDs should be attempted, with necessary precaution for those with gastrointestinal risk factors. Opioids can be effective in patients who have failed or cannot tolerate paracetamol or NSAIDs, with necessary precaution for those at risk of drug abuse or dependence. Glucosamine, chondroitin, ASU, diacerein, and hyaluronic acid.
- Invasive interventions. These include intra-articular injections, lavage, and joint replacement. Intra-articular injections can help with knee pain flares associated with effusion. Joint replacement should be considered for patients with refractory pain and disability who have radiographic evidence of knee osteoarthritis.
Special Considerations and contraindications to total knee replacement
The mortality following total knee replacement is about 1.5% annually. However, the majority of these procedures are performed in the elderly and this figure must be viewed in the context of this patient population. The most important risks associated with total knee replacement are superficial infection (3.9%), deep infection (1.7%), pulmonary embolism (2%), deep vein thrombosis (6.5%), and peripheral nerve damage (2.1%). At 4 years follow-up the average rate of total knee replacement revision is 3.8%.5 Older patients experience similar improvements in clinical outcomes compared with younger patients. Thus, age should not be used as a contraindication to surgery, and patients should be evaluated based on the criteria above for severity of joint disease to determine their surgical candidacy. Patients should be aware that men report greater improvements in postoperative pain compared with women.6
Absolute contraindications for total knee replacement include active or latent knee sepsis, presence of active infection in other parts of the body, extensor mechanism dysfunction, patient's inability to tolerate procedure.
Relative contraindications include:9
- Morbid obesity due to higher rate of perioperative complications, particularly wound drainage, infections, and medial collateral ligament avulsion.
- Neuropathic arthropathy due to higher rate of complication and failure.
- Post-traumatic arthritis and prior history of infection.
- Severe peripheral vascular disease.
- Poor patient motivation or unrealistic expectation.
- Noncompliance due to major psychiatric disorder, alcohol, or drug abuse.
- Muscle weakness or insufficient bone stock for reconstruction.
Pre-op X-Rays

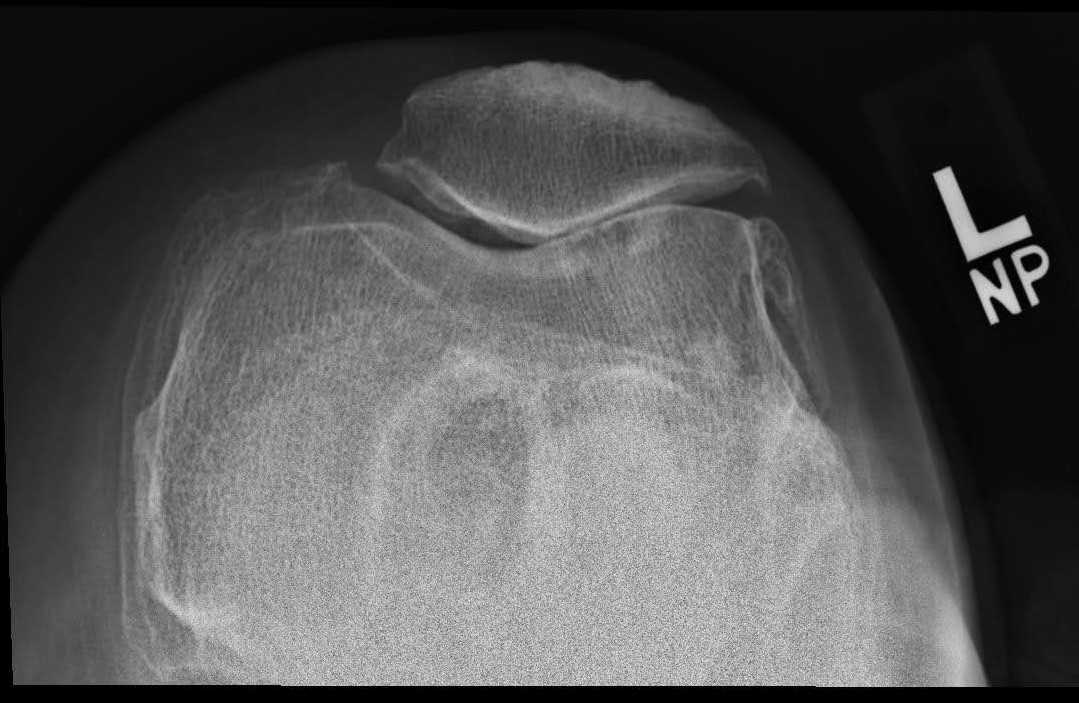
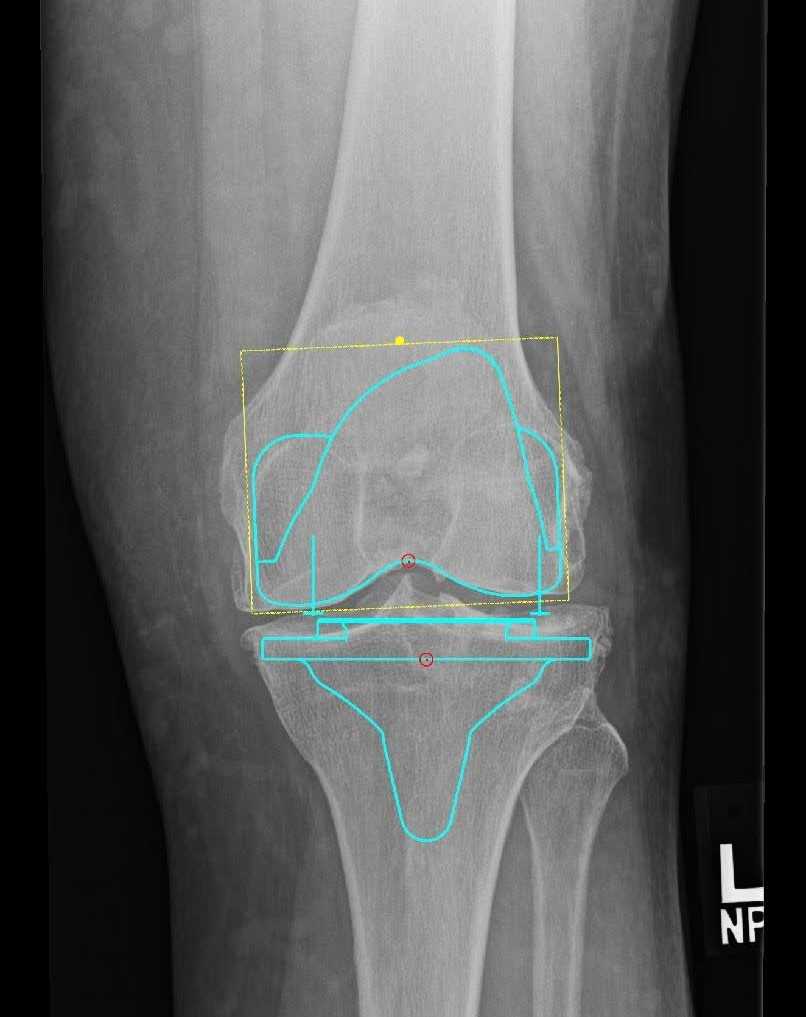

Figure 1. Pre-op x-rays.
Discussion
Total knee replacement when indicated for the treatment of degenerative joint disease can provide significant pain relief and improved quality of life. This procedure is usually performed following failed trials of less-invasive measures, which include lifestyle modification, pharmacologic therapy, and injection therapy. Following total knee replacement, patients report good clinical outcomes and improved quality of life. All patients should be aware that, as with all surgical procedures, there are risks involved. These risks may be serious and include surgical site infection, pulmonary embolism, deep vein thrombosis, nerve damage, and the need for further procedures. The decision to undergo total joint replacement should be done in partnership between the patient and surgeon, weighing the benefits and risks of the procedure and with an appreciation for the expected outcome.
Overall Outcomes After Total Knee Arthroplasty
Among patients who undergo total knee replacement, nearly 90% report a good or excellent outcome after 4 years of follow-up with an average 8-degree improvement in range of motion. With regard to pain improvement, 75% of patients report no postoperative pain and 20% report only mild postoperative pain at 4 years follow-up.5,6 Notably, patients who report a worse quality of life preoperatively are likely to experience the greatest improvement as a result of total knee replacement. Patients who have undergone total joint replacement report quality of life nearly equivalent to healthy control groups. At one-year follow-up, total knee recipients report improved energy, emotion, sleep, and mobility.6
Future Research
Future research may focus on investigating improved methods for controlling postoperative pain, risk factors for surgical complications including infection and revision procedures, and the optimal methods for minimizing these risks.
Equipment
- Attune system with a size 4 femoral component
- Size 5 tibia with 4x7 fixed bearing cruciate retaining insert
- 38 mm all polyethylene patellar button
- Tourniquet
Disclosures
The author certifies that he, or a member of his immediate family, has or may receive payments or benefits, during the study period, an amount of more than USD 1,000,001 from DePuy (Warsaw, IN, USA).
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Skou ST, Roos EM, Laursen MB, et al. A randomized, controlled trial of total knee replacement. N Engl J Med. 2015;373(17):1597-1606. doi:10.1056/NEJMoa1505467.
-
Kohn MD, Sassoon AA, Fernando ND. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin Orthop Relat Res. 2016 Aug;474(8):1886-93. doi:10.1007/s11999-016-4732-4.
- Moseng T, Vliet Vlieland TPM, Battista S, et al. EULAR recommendations for the nonpharmacological core management of hip and knee osteoarthritis: 2023 update. Ann Rheum Dis. Published online January 11, 2024. doi:10.1136/ard-2023-225041.
-
Driban JB, Harkey MS, Barbe MF, et al. Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review. BMC Musculoskelet Disord. 2020 May 29;21(1):332. doi:10.1186/s12891-020-03367-2.
- Rathod J, Agarwal K. Functional outcome of bilateral total knee replacement arthroplasty in bilateral tricompartmental osteoarthritis of knee. Int J Orthop Sci. 2021;7(1):998-1005. doi:10.22271/ortho.2021.v7.i1o.259.
- Canovas F, Dagneaux L. Quality of life after total knee arthroplasty. Orthop Traumatol Surg Res. 2018;104(1S):S41-S46. doi:10.1016/j.otsr.2017.04.017.
- Judge A, Arden NK, Cooper C, et al. Predictors of outcomes of total knee replacement surgery. Rheumatology (Oxford). 2012;51(10):1804-1813. doi:10.1093/rheumatology/kes075.
- Sunadi A; Nursalam; Mustikasari; Krisnana I, Kurniawati ND. Factors Correlated with the Quality of Life after Total Knee Arthroplasties: A Literature Review. Malays Orthop J. 2024 Mar;18(1):1-10. doi:10.5704/MOJ.2403.001.
- Hsu H, Siwiec RM. Knee Arthroplasty. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
- Parvizi J, Klatt B, eds. Essentials in Total Knee Arthroplasty. 1st ed. Boca Raton, FL: CRC Press; 2011.

.jpg)
| Publication Date | 10/21/2024 |
| Article ID | 13 |
| Production ID | 0076 |
| Volume | 2024 |
| Issue | 13 |
| DOI | |
| https://doi.org/10.24296/jomi/13 | |