Pancreatic Debridement via Sinus Tract Endoscopy
Abstract
Sinus tract endoscopy (STE) is a minimally-invasive technique for debridement of dead or infected tissue. STE is usually used for treatment of infected pancreatic or peripancreatic necrosis, though other applications have been described. STE involves placement of a percutaneous drain followed by fluoroscopically-guided dilation of the drain tract to allow for placement of a working sheath. An endoscope is then introduced through the sheath and used to debride necrotic tissue. A drain is then replaced through the same tract at the conclusion of the procedure. In this case we use STE to debride infected peripancreatic necrosis caused by a traumatic pancreatic injury and complicated by an enteric fistula.
Case Overview
Background
Acute pancreatitis affects over 275,000 people per year in the United States. Approximately 20% develop necrosis and 10-20% of those develop infected necrosis. Infected pancreatic or peripancreatic necrosis is the primary indication for intervention in necrotizing pancreatitis.1, 2
Focused History of Patient
Our patient is a 58-year-old male who was involved in a motor vehicle collision and suffered multiple injuries including to the pancreas. He was initially managed at another hospital where he underwent endoscopic retrograde cholangiopancreatography and pancreatic duct stenting. He developed a symptomatic acute peripancreatic fluid collection and underwent percutaneous drainage, which revealed infection. When his peripancreatic collection did not resolve, his drains were upsized. An inferior left retroperitoneal collection improved significantly, but he developed a persistent necrotic collection adjacent to the pancreatic tail that did not improve with percutaneous drainage. A fluoroscopic drain injection demonstrated that the collection communicated with the small bowel. He had persistent abdominal pain and was intermittently febrile and so was referred to us.
Physical Exam
Physical exam revealed a healthy-appearing man with normal vital signs. Head, neck, and cardiopulmonary exam were all normal. His abdomen was soft and mildly tender in the left hemiabdomen. He had two 24 Fr drains protruding from the lateral abdomen with purulent output.
Imaging
An abdominal CT scan showed a persistent 9 cm by 6 cm collection of walled-off necrosis adjacent to the pancreatic tail in the left upper quadrant (Figure 1).
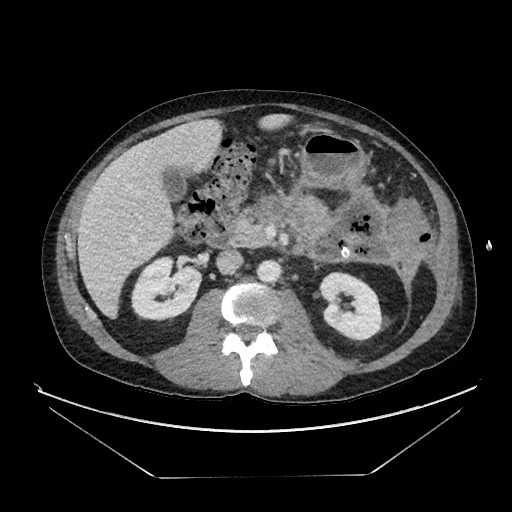
Figure 1. CT scan of the patient showing a necrotic collection in the vicinity of the pancreatic tail containing air and with percutaneous drain present.
Natural History
Most peripancreatic necrosis results from acute pancreatitis, which is most commonly caused by ethanol use or gallstones. Trauma-induced necrosis such as in this case is relatively rare. Most pancreatitis is mild and does not result in local complications such as peripancreatic fluid collections or necrosis. When these occur, they should be managed non-interventionally at first, and necrosis or fluid collections will resolve in the majority of cases. When necrosis or fluid collections persist, they are at risk for infection as in this case. When infection occurs, it should be managed using a step-up approach in which a minimally invasive drainage procedure (either endoscopic or percutaneous) is the first step. 20–40% of the time this will resolve the infection. When it does not, necrosectomy is generally required.2–4
Options for Treatment
At the time of presentation to us, there were several options for the patient. Continued percutaneous drainage might have eventually resolved the collection in this case but at the cost of many weeks of ongoing external drainage. This patient’s necrotic collection was not amenable to transgastric drainage, as it did not abut the stomach. Video-assisted retroperitoneal debridement (VARD) or sinus tract endoscopy (STE) are minimally-invasive options for this patient. Open surgical necrosectomy would also have been possible.
Rationale for Treatment
We chose STE in this case because the total size of the collections was relatively small, and the presence of enteric fistulae increased the chance of wound complications, which would be minimized by STE.
Discussion
Recent years have seen a shift from open surgery to a minimally-invasive, step-up approach for the treatment of infected pancreatic necrosis.2–4 This article describes STE, one important technique of minimally-invasive necrosectomy.5 The step-up approach and use of STE and other minimally-invasive techniques has significantly decreased morbidity and mortality for patients undergoing intervention for infected pancreatic necrosis.6 Regardless of the exact technique employed, the common management principles include early non-interventional management to allow the necrosis to wall off, initial intervention with minimally-invasive drainage, and minimally-invasive necrosectomy addressing clearly demarcated necrosis.
While this article demonstrates the use of STE for treatment of infected peripancreatic necrosis, it is important to understand what other techniques are available to optimize STE. The main other techniques utilized are VARD and transgastric necrosectomy, which can be performed endoscopically or surgically. VARD requires a retroperitoneal window into the necrosis and is optimally suited to quick debridement of large-volume necrosis tracking to the paracolic gutters. It involves a cutdown performed over the drain to access the necrosis cavity.7 Transgastric necrosectomy is a preferred route when there is a clear transgastric window into the necrosis cavity with the majority of the necrosis burden in continuity with the posterior stomach. Endoscopic transgastric drainage and debridement and VARD have been favorably compared with open necrosectomy in two recent randomized trials.3,8,9 Both were shown to reduce the incidence of new-onset organ failure after debridement. Endoscopic debridement also resulted in a reduction in mortality and external fistula formation compared with surgical necrosectomy. Its main disadvantages are the anatomic requirements for transgastric access and the frequent need for multiple reinterventions (median 3, in two different randomized trials).9,10 VARD performed as part of a step-up protocol resulted in lower costs and lower rates of diabetes mellitus compared with necrosectomy performed via laparotomy but did not produce a mortality benefit nor reduce the rate of fistula formation.8 VARD and endoscopic transgastric necrosectomy have now been directly compared with each other in a head-to-head randomized trial, which showed no difference in death or major complications but an advantage for endoscopic necrosectomy in some secondary endpoints including pancreatic fistula.10
Surgical transgastric necrosectomy can be done open or laparoscopically, obviates the need for multiple procedures, and allows for simultaneous cholecystectomy when needed in cases of biliary pancreatitis. However, it is still subject to the same anatomic constraints as endoscopic transgastric necrosectomy. A recent randomized trial comparing a combination of surgical transgastric necrosectomy with VARD showed higher complication rates with the surgical approaches but no difference in mortality.11 Although this did not directly compare surgical with endoscopic transgastric approaches, it does suggest that the surgical approach should be used selectively. Combining endoscopic transgastric drainage with percutaneous drainage, termed “dual modality drainage” (DMD), accrues the chief benefit of endoscopic drainage—the low rate of external fistula—but also allows access to portions of the collections that may be difficult to reach endoscopically.12 In the original description of DMD, no necrosectomy was performed by either route. We now routinely combine transgastric drainage with necrosectomy performed by either STE or VARD.13 We have found that this combines the main advantages of surgical necrosectomy (rapid debridement and the ability to more easily access necrosis not adjacent to the stomach) and endoscopic transgastric necrosectomy (control of external fistulae).
When considering VARD versus STE, each has advantages and disadvantages. VARD uses equipment familiar to surgeons, such as a laparoscope for visualization and ring or laparoscopic forceps for debridement, and the actual act of debridement once the cavity is entered is very similar to open surgical necrosectomy. For these reasons, many surgeons may find it to be an easier technique to adopt. VARD, like open necrosectomy, allows rapid debridement of large chunks of necrosis, and in our experience, has not yet required repeated procedures. There are two main disadvantages to VARD. One is that wound complications, while generally minor, are relatively common. The other is the requirement for a retroperitoneal pathway into the necrosis that is wide enough to allow a safe cutdown along the drain tract and also enters the cavity in a location that allows for complete debridement.
Compared with VARD or endoscopic transgastric drainage, STE is relatively free of anatomic requirements. Virtually any necrotic collection that can be accessed percutaneously can be accessed by STE. This is an advantage when the only or best route into the necrosis is transperitoneal, intercostal, or when the window into the necrosis is so narrow that the cutdown required for VARD risks damage to vital structures. This flexibility is perhaps the biggest benefit of STE, as it greatly expands patient eligibility and obviates the need for either a more morbid open necrosectomy or very prolonged percutaneous drainage for the treatment of collections inaccessible via transgastric or retroperitoneal approaches. Additionally, STE is essentially free of wound complications, since the only incision is the actual drain site. However, STE requires familiarization with equipment used less frequently by surgeons, such as a rigid nephroscope and intraoperative fluoroscopy. The relatively small instrumentation required also means that for large necrotic collections, multiple procedures are frequently required.
In this case, with a relatively small collection of necrosis, complete debridement was accomplished in one procedure. When this is not possible due to a large volume of necrosis or due to tight adherence of the necrosis to vital structures such as splenic vessels, a drain can be left in place with a repeat procedure planned. If a repeat procedure is planned, we place a 7 Fr catheter adjacent to the larger drainage catheter through the same skin incision through which to instill irrigation. We typically perform continuous irrigation with 0.9% saline at 200 ml/hour for 48–72 hours between procedures. If present, the irrigation catheter can be attached to an infusion pump, and the drainage catheter is connected to a drainage bag, and the skin is closed with interrupted sutures around the catheter. After a period of irrigation, it is very common to find that residual necrosis is loosely adherent and much more quickly and safely debrided than would have been possible by persisting at the initial procedure. For this reason, the temptation to aggressively debride the walls of the cavity should be avoided due to the risk of bleeding, and the threshold to repeat the procedure should be low. Even following this guideline, our median number of procedures remains 1 with a mean of 1.8 (range 1–4).7
Finally, this case illustrates an enteric fistula to the jejunum. Enteric fistulae to the small bowel, stomach, and colon are not uncommon. To date, we have never needed to intervene directly on the fistula, and all fistulae have closed with complete debridement of the necrosis cavity, as in this case. Surgical repair or resection of the proximal bowel or diversion (in the case of distal small bowel or colonic fistulae) should be used very selectively. This patient was discharged home the day after the procedure. His drains were removed on postoperative day 12.
Equipment
- Radiolucent operating room table
- C-arm
- Amplatz Super Stiff Guidewire (.035” diameter), Boston Scientific
- High Pressure Nephrostomy Balloon Catheter and Sheath (30 Fr), Boston Scientific
- Rigid Nephroscope (30 Fr), Storz
- 16-28 Fr percutaneous drain
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Peery AF, Crockett SD, Barritt AS, et al. Burden of gastrointestinal, liver, and pancreatic diseases in the United States. Gastroenterology. 2015;149(7):1731-1741. doi:10.1053/j.gastro.2015.08.045.
- Tenner S, Baillie J, DeWitt J, Vege SS; American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108(9):1400-1416. doi:10.1038/ajg.2013.218.
- Hollemans RA, Bakker OJ, Boermeester MA, et al.; Dutch Pancreatitis Study Group. Superiority of step-up approach vs open necrosectomy in long-term follow-up of patients With necrotizing pancreatitis. Gastroenterology. 2019;156(4):1016-1026. doi:10.1053/j.gastro.2018.10.045.
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 suppl 2):e1-15. doi:10.1016/j.pan.2013.07.063.
- Carter CR, McKay CJ, Imrie CW. Percutaneous necrosectomy and sinus tract endoscopy in the management of infected pancreatic necrosis: an initial experience. Ann Surg. 2000;232(2):175-180. doi:10.1097%2F00000658-200008000-00004.
- van Brunschot S, Hollemans RA, Bakker OJ, et al. Minimally invasive and endoscopic versus open necrosectomy for necrotising pancreatitis: a pooled analysis of individual data for 1980 patients. Gut. 2018;67(4):697-706. doi:10.1136/gutjnl-2016-313341.
- Fong ZV, Fagenholz PJ. Minimally invasive debridement for infected pancreatic necrosis. J Gastrointest Surg. 2019;23(1):185-191. doi:10.1007/s11605-018-3908-5.
- van Santvoort HC, Besselink MG, Bakker OJ, et al.; Dutch Pancreatitis Study Group. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med. 2010;362(16):1491-1502. doi:10.1056/NEJMoa0908821.
- Bakker OJ, van Santvoort HC, van Brunschot S, et al.; Dutch Pancreatitis Study Group. Endoscopic transgastric vs surgical necrosectomy for infected necrotizing pancreatitis: a randomized trial. JAMA. 2012;307(10):1053-1061. doi:10.1001/jama.2012.276.
- van Brunschot S, van Grinsven J, van Santvoort HC, et al.; Dutch Pancreatitis Study Group. Endoscopic or surgical step-up approach for infected necrotising pancreatitis: a multicentre randomised trial. Lancet. 2018;391(10115):51-58. doi:10.1016/S0140-6736(17)32404-2.
- Bang JY, Arnoletti JP, Holt BA, et al. An endoscopic transluminal approach, compared with minimally invasive surgery, reduces complications and costs for patients with necrotizing pancreatitis. Gastroenterology. 2019;156(4):1027-1040.e3. doi:10.1053/j.gastro.2018.11.031.
- Ross AS, Irani S, Gan SI, et al. Dual-modality drainage of infected and symptomatic walled-off pancreatic necrosis: long-term clinical outcomes. Gastrointest Endosc. 2014;79(6):929-935. doi:10.1016/j.gie.2013.10.014.
- Fagenholz PJ, Thabet A, Mueller PR, Forcione DG. Combined endoscopic trangastric drainage and video assisted retroperitoneal pancreatic debridement - the best of both worlds for extensive pancreatic necrosis with enteric fistulae. Pancreatology. 2016;16(5):788-790. doi:10.1016/j.pan.2016.06.009.

| Publication Date | 1/14/2021 |
| Article ID | 250 |
| Production ID | 0250 |
| Volume | 2021 |
| Issue | 250 |
| DOI | |
| https://doi.org/10.24296/jomi/250 | |