Vaginal Hysterectomy, Uterosacral Ligament Suspension, Anterior Repair, and Perineorrhaphy
Abstract
The patient is a 74-year-old female who presented with bothersome stage III pelvic organ prolapse. She desired definitive surgical management for her prolapse and opted for total vaginal hysterectomy, uterosacral ligament suspension, and anterior/posterior vaginal repairs. She had urodynamic testing before the surgery that showed no stress urinary incontinence, no detrusor overactivity, and normal bladder capacity. The surgery was uncomplicated. She was discharged home the same day as surgery, and her postoperative recovery was unremarkable.
Case Overview
Background
The patient is a 74-year-old female with a past medical history of hypertension and type 2 diabetes mellitus (on metformin) who presented with symptoms of bothersome vaginal bulge that she had to manually reduce. She had urinary hesitancy and at times would have to lean forward to initiate voiding. She denied symptoms of urinary incontinence and was not sexually active. She had a history of 3 spontaneous vaginal deliveries, the largest of which was 7 lb 7 oz.
Physical Exam
A pelvic exam was performed in the dorsal lithotomy position. With Valsalva, the anterior vaginal wall prolapsed 2 cm below the hymen, the cervix 3 cm above the hymen, and the posterior wall 2 cm above the hymen. The vaginal length was 9 cm. Empty supine cough stress test was negative for urinary leakage. See Figure 1 for graphic demonstration of prolapse.
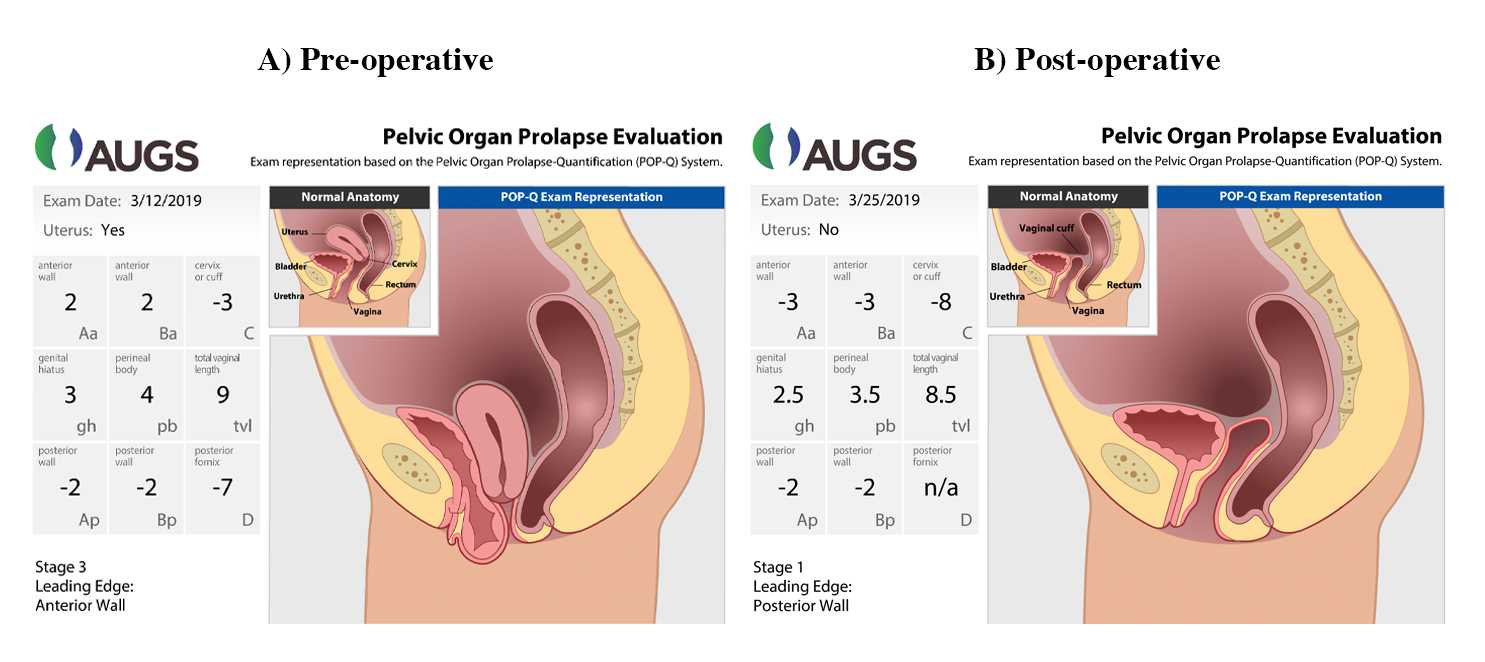
Figure 1. Graphic Demonstration of Pre- and Postoperative POP-Q Measurements
Used with permission from the American Urogynecologic Society (AUGS).
Imaging
There was no indication for imaging for this patient.
Other Testing
She had urodynamic testing that did not demonstrate occult stress urinary incontinence (SUI). Based on this testing, it was recommended that she not undergo an anti-incontinence procedure at the time of the surgical correction of pelvic organ prolapse.
As a non-frail 74-year-old woman, preoperative labs included complete blood count (CBC), hemoglobin A1c (Hgb A1C), urinalysis, urine culture, and electrocardiogram (ECG). She was not anemic or thrombocytopenic, Hgb A1C was 6.2 mg/dl, and urine was without evidence of infection. ECG showed a normal sinus rhythm. The patient was thus cleared for surgery.
Options for Treatment
Treatment of prolapse depends on the patient’s goals and preferences. Options include expectant management, pelvic floor physical therapy, a pessary, and surgical management. The patient had symptomatic, bothersome prolapse and declined conservative therapy. She desired definitive surgical management.
Surgical options for apical pelvic organ prolapse include:
- Vaginal repair using native tissue: It includes either a uterosacral ligament suspension or sacrospinous ligament fixation. This procedure can also include a vaginal hysterectomy, as well as anterior and/or posterior vaginal repairs. Success rates range from 81–98%.1 The risk of injury to bowel or bladder is 0–2%.1
- Laparoscopic or robotic sacrocolpopexy: It uses polypropylene mesh to resuspend the vagina. This procedure can also include a hysterectomy. The risk of recurrent prolapse is approximately 7%, but there is a slightly higher risk of urinary or bowel injury at 0–4%.2
- Colpocleisis: an obliterative procedure that is accomplished by suturing the anterior vaginal wall to the posterior vaginal wall, closing the upper two-thirds of the vaginal canal. This procedure precludes vaginal intercourse. It is very durable; the risk of recurrent prolapse is approximately 0–2%.3
Rationale for Treatment
The patient desired a native tissue reconstructive procedure. She declined augmentation with a graft.
Special Considerations
As described above, the patient did undergo urodynamic testing to assess for occult SUI, which is stress urinary incontinence that is “unmasked” by the prolapse repair. During the testing, the prolapse is elevated to simulate the surgical repair, and the patient is taken through various maneuvers to elicit SUI. If the patient does have SUI during testing, she is more likely to have SUI after the prolapse repair.4 However, there is a possibility that the patient may have leaking even if the testing is negative and may require a separate staged procedure to address the incontinence.4 A risk calculator is available for estimating the risk of de novo postoperative SUI after the surgery for pelvic organ prolapse.5
Discussion
The patient was taken to the operating room where general anesthesia was given. She was intubated with an endotracheal tube. She received subcutaneous heparin as venous thromboembolism prophylaxis and IV cefazolin as antibiotic prophylaxis. She was placed in the dorsal lithotomy position in Yellow-Fin stirrups.
The hysterectomy was performed first. A Foley catheter was placed into the bladder, and the Lone Star self-retaining retractor (Cooper Surgical) was utilized for retraction. Jacobson clamps were used to grasp the cervix, and a dilute solution of Marcaine with epinephrine was injected circumferentially around the cervix. Using Bovie cautery, a circumferential incision was made around the cervix. The posterior cul-de-sac was then entered sharply, and a weighted speculum was placed in the posterior cul-de-sac. The uterosacral ligaments were then clamped, cut, and suture-ligated bilaterally. These sutures were held. An attempt was made to enter the anterior cul-de-sac, but this was not yet possible so the LigaSure Impact open instrument (Medtronic USA) was used to coagulate and cut the cardinal ligament, taking the uterine vessels in the process. The vesicouterine peritoneum was identified and entered sharply. A retractor was placed anteriorly to protect the bladder. Using the LigaSure, the utero-ovarian vascular bundle was coagulated and cut. The uterus was then handed off for a permanent section. The adnexa was palpated and felt normal. The pedicles were then inspected, and excellent hemostasis was noted.
The bowel was packed away with moist laparotomy sponges. The right side of the posterior vaginal cuff was grasped with a long Allis and put on tension in order to visually locate the right uterosacral ligament. Two 0-polydioxanone (PDS) sutures were then anchored into the uterosacral ligament approximately 1–2 cm above the level of the ischial spine. The same procedure was then performed on the left side. The four PDS sutures were then held on tension while cystoscopy was performed, and bilaterally brisk ureteral efflux was confirmed.
Attention was then turned to the anterior colporrhaphy. Allis clamps were placed along the midline of the anterior vaginal wall, and dilute Marcaine with epinephrine was injected along the anterior vaginal wall. A vertical midline incision was made along the anterior vaginal wall, and the epithelium was dissected off of the underlying tissue using Metzenbaum scissors. Plication of the underlying vaginal muscularis and adventitia was performed using a running delayed absorbable suture. Redundant vaginal mucosa was trimmed, and the vaginal incision was closed with a delayed absorbable suture. The uterosacral ligament suspension sutures were then placed through the vaginal apex bilaterally and held. The vaginal cuff was closed with a delayed absorbable suture in a vertical fashion. The uterosacral ligament suspension sutures were tied, thus suspending the vaginal apex. Cystourethroscopy was performed, and the bladder was inspected. There were no lesions, tumors, or stones seen in the bladder. Bilateral ureteral efflux was visualized with prior-given phenazopyridine. Urethral integrity was confirmed.
Attention was then turned to the perineorrhaphy and posterior colporrhaphy. The posterior hymen was grasped on both sides with Allis clamps to allow entry of three fingers. The area of anticipated dissection was then injected with 0.25% Marcaine with epinephrine. A diamond-shaped incision was then made over the perineal body skin and posterior vaginal epithelium. A midline vaginal incision was then made from the perineum to the proximal border of the rectocele. The vaginal epithelium was then dissected off of the underlying rectovaginal connective tissue. The rectovaginal fibromuscular layer was then plicated in the midline using delayed absorbable suture in a running fashion. The excess vaginal epithelium was trimmed. The bulbocavernosus muscles were plicated in the midline with interrupted 0-polyglactin suture followed by the transverse perineal muscles. The midline incision was then closed in a running fashion using a delayed absorbable suture. The rectal exam confirmed no injury to the rectum.
Postoperative Course
Approximately two hours after surgery, the patient underwent a backfill voiding trial. The bladder was filled via the Foley catheter with 300 ml of sterile water. The Foley catheter was removed, and the patient was able to void more than 200 ml, thus passing the trial of void. Subsequently, she met all discharge criteria and was discharged home on the day of surgery. We send more than 90% of our patients home on the day of surgery with our Enhanced Recovery After Surgery protocol.
Despite the fact that most patients undergoing vaginal hysterectomies can be successfully discharged on the same day of surgery,6 up to one-third of such patients may be required to stay overnight because of mild postoperative complications such as prolonged post-anesthesia effects.7
The patient was seen at two weeks and seven weeks after surgery. She was doing well at both of those visits and denied any prolapse, incontinence, or voiding dysfunction. See Figure 1B for postoperative POP-Q measurements.
Equipment
- Lone Star self-retaining retractor (Cooper Surgical)
- Heaney curved hysterectomy clamp
- LigaSure Impact open instrument (Medtronic USA)
- Cystoscopy equipment with 70-degree lens in order to see ureteral jets
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Margulies RU, Rogers MAM, Morgan DM. Outcomes of transvaginal uterosacral ligament suspension: systematic review and metaanalysis. Am J Obstet Gynecol. 2010;202(2):124-134. doi:10.1016/j.ajog.2009.07.052.
- Nosti PA, Andy UU, Kane S, et al. Outcomes of abdominal and minimally invasive sacrocolpopexy: a retrospective cohort study. Female Pelvic Med Reconstr Surg. 2014;20(1):33-37. doi:10.1097/spv.0000000000000036.
- Zebede S, Smith AL, Plowright LN, Hegde A, Aguilar VC, Davila GW. Obliterative LeFort colpocleisis in a large group of elderly women. Obstet Gynecol. 2013;121(2 part 1):279-284. doi:10.1097/AOG.0b013e31827d8fdb.
- Visco AG, Brubaker L, Nygaard I, et al. Pelvic floor disorders network. the role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the colpopexy and urinary reduction efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):607-614. doi:10.1007/s00192-007-0498-2.
- Jelovsek JE, Chagin K, Brubaker L, et al. Pelvic floor disorders network. a model for predicting the risk of de novo stress urinary incontinence in women undergoing pelvic organ prolapse surgery. Obstet Gynecol. 2014;123(2 part 1):279-287. doi:10.1097/AOG.0000000000000094.
- Zakaria MA, Levy BS. Outpatient vaginal hysterectomy: optimizing perioperative management for same-day discharge. Obstet Gynecol. 2012;120:1355-61. doi:10.1097/AOG.0b013e3182732ece.
- Liu L, Yi J, Cornella J, Butterfield R, Buras M, Wasson M. Same-day discharge after vaginal hysterectomy with pelvic floor reconstruction: pilot study. J Minim Invasive Gynecol. 2019 Apr 10;27(2):498-503. doi:10.1016/j.jmig.2019.04.010.



| Publication Date | 5/4/2023 |
| Article ID | 267 |
| Production ID | 0267 |
| Volume | 2023 |
| Issue | 267 |
| DOI | |
| https://doi.org/10.24296/jomi/267 | |