The Versatile Latissimus Dorsi Muscle as a Local Flap for Chest Wall Coverage
Abstract
Not only is the skin the largest organ by the surface area of the body, the integument has multiple essential functions such as preventing dehydration, acting as a first-line barrier to infection, permitting unrestricted movement of joints, as well as sustaining a normal profile and appearance. Occasionally, the treatment of breast cancer requires the removal of the breast while also leaving a large chest skin deficit. Especially if radiation has been done or is planned, the best way to restore the missing skin to preserve its essential function would be by the use of a vascularized flap. Sometimes this can be achieved while simultaneously providing a reconstruction of a very aesthetic breast mound. Depending on circumstances and the extent of disease, a simpler solution might be to just close only the chest wound that has been created. A “workhorse” flap alternative that is almost always available to achieve this is the latissimus dorsi (LD) muscle from the back, as this can be moved to almost all regions of the chest. The LD muscle usually can be swung to the chest about its blood vessels that remain attached to the armpit, and so would be called a local flap that as such avoids the complexities of a transfer requiring microsurgery to reconnect the blood supply. The long-term experience by reconstructive surgeons in using the LD muscle as a local flap, not just for the chest but also the back, head, and neck, has proven its deserved accolade to be a versatile flap unparalleled by most other donor sites.
Case Overview
This moderately-aged female apparently had had a previous lumpectomy with postoperative radiation therapy for left breast cancer, but subsequently developed a local recurrence. Her general surgeon now recommended removal of the entire left breast including the involved overlying skin. Such a procedure would leave a large hole in her chest that could not be reliably closed by just bringing the remaining skin edges together, as they had been irradiated, which is known to impede if not prevent normal wound healing.1 A simple skin graft would be a dangerous solution, as a graft has no blood supply of its own and instead relies on nutrition from the tissue upon which it is placed, where here as stated was already precarious. Instead, a flap, which is tissue that always has an intact blood supply of its own, becomes essential.
In planning the surgical cure for the patient, the general surgeon asked the plastic surgeons to be ready to help as needed, as they are accustomed to moving flaps from one body region to another. The best way to do this should be the simplest and most reliable, which is selecting a flap from nearby the mastectomy site as what would be called a local flap. A “workhorse” option in this situation is the latissimus dorsi (LD) muscle from the back,2 as this is a very large muscle that is expendable, meaning that loss of its function is usually inconsequential.3 The LD muscle blood supply comes from vessels found in the armpit (Figure 1), so that with (as a so-called musculocutaneous flap) or without the overlying skin, it can be swung like a pendulum attached only by its blood vessels—from the back to anywhere on the chest!
A major operation like this as planned is known to take 3–4 hours and would be extremely painful without general anesthesia, requiring the patient to be put asleep. After the general surgeon removed the breast, indeed a large 9x13-cm defect requiring skin replacement was present. Next, the plastic surgeons began the reconstruction seen in this video. A similarly-sized design on the skin of the back was made toward the waist, where it remained attached to the LD muscle. The skin and muscle together were then raised from the back, proceeding toward the armpit as far as necessary while constantly watching so as not to injure the blood supply, until the flap could be passed without tension through a subcutaneous tunnel to reach the mastectomy wound. There it was inset to close the chest wound, while the donor site of the back could also be closed directly. Afterward, the patient required admission to the hospital due to the extent of the surgery and to monitor the flap to make sure its circulation was never compromised, as proved to be the case.

Figure 1. The circulation to the large, flat-contoured, LD muscle can almost in its entirety be via its dominant pedicle, the thoracodorsal vessels (on green microgrid).
Discussion
More often than not today, the plastic surgeon following a mastectomy is requested to perform a breast reconstruction that will provide usually a very aesthetic facsimile of the original. Most commonly when a flap is chosen, this is done as a perforator flap from the patient’s own abdomen as what is called an autogenous tissue transfer, and it is called the deep inferior epigastric perforator (DIEP) flap.4 In addition, the patient gets a concomitant “tummy tuck” as a bonus. However, this requires joining small blood vessels together under the microscope, which is a skill not available in all locations. One secondary option has been to transfer the LD muscle from the back as a local flap to cover a silicone breast implant,5 or to take the skin overlying that muscle as a so-called musculocutaneous flap, which, if thick enough, can even avoid the use of an implant.6
Sometimes, as in this case, the goal is more limited, and just healing the chest wound is sought. Especially after irradiation has prevented the use of the muscles from the anterior chest, the LD muscle still typically remains as a suitable option as a local flap to simply achieve this objective (Figure 2). Whereas microsurgical tissue transfer requiring the anastomosis of small vessels has been a routine for a mere 50 years,7 the Italian Tansini actually described the LD musculocutaneous flap in 1906 as his solution to close the difficult mastectomy defect!8 Although today the skin of the LD flap can be transferred without the muscle as what is called a “perforator flap” so as to preserve function,9 this is much more tedious and difficult to accomplish than to just include the muscle itself, and preferably should be restricted to a surgeon experienced in that variation. Indeed, the LD muscle, or musculocutaneous flap, remains even today a truly versatile flap due to its consistent anatomy, ease of harvest, and extended reach as a local flap.2
A B C
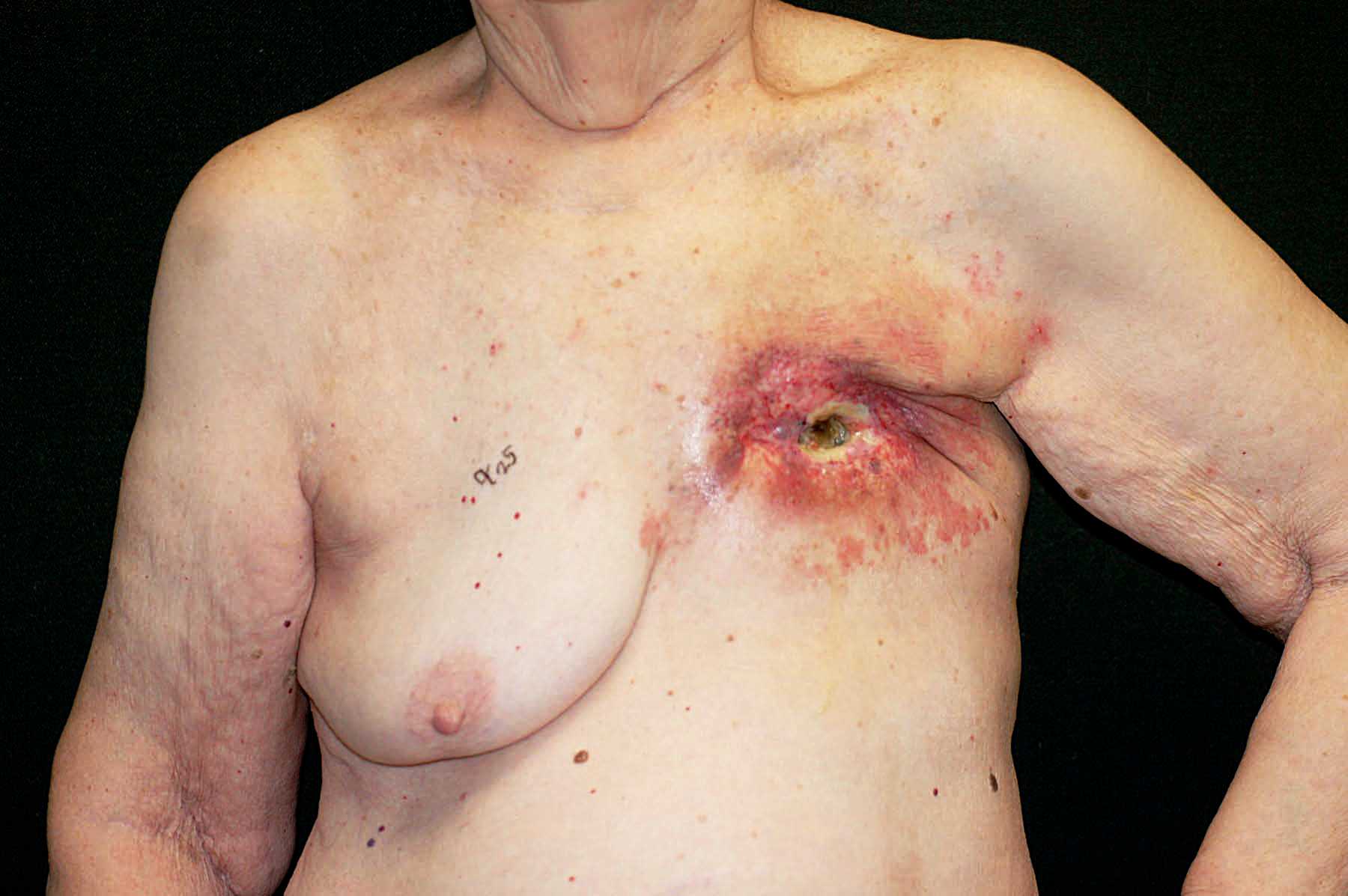
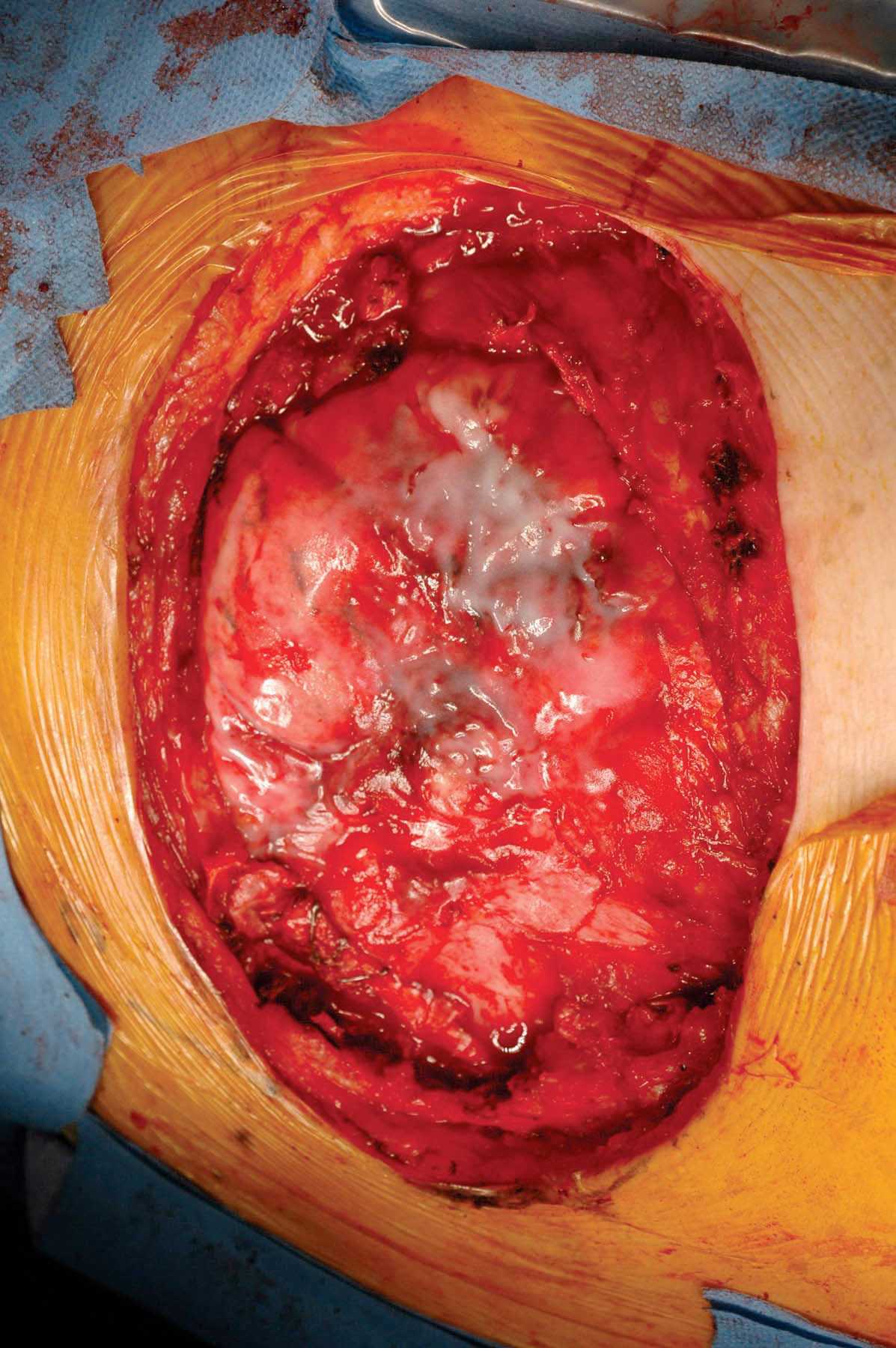
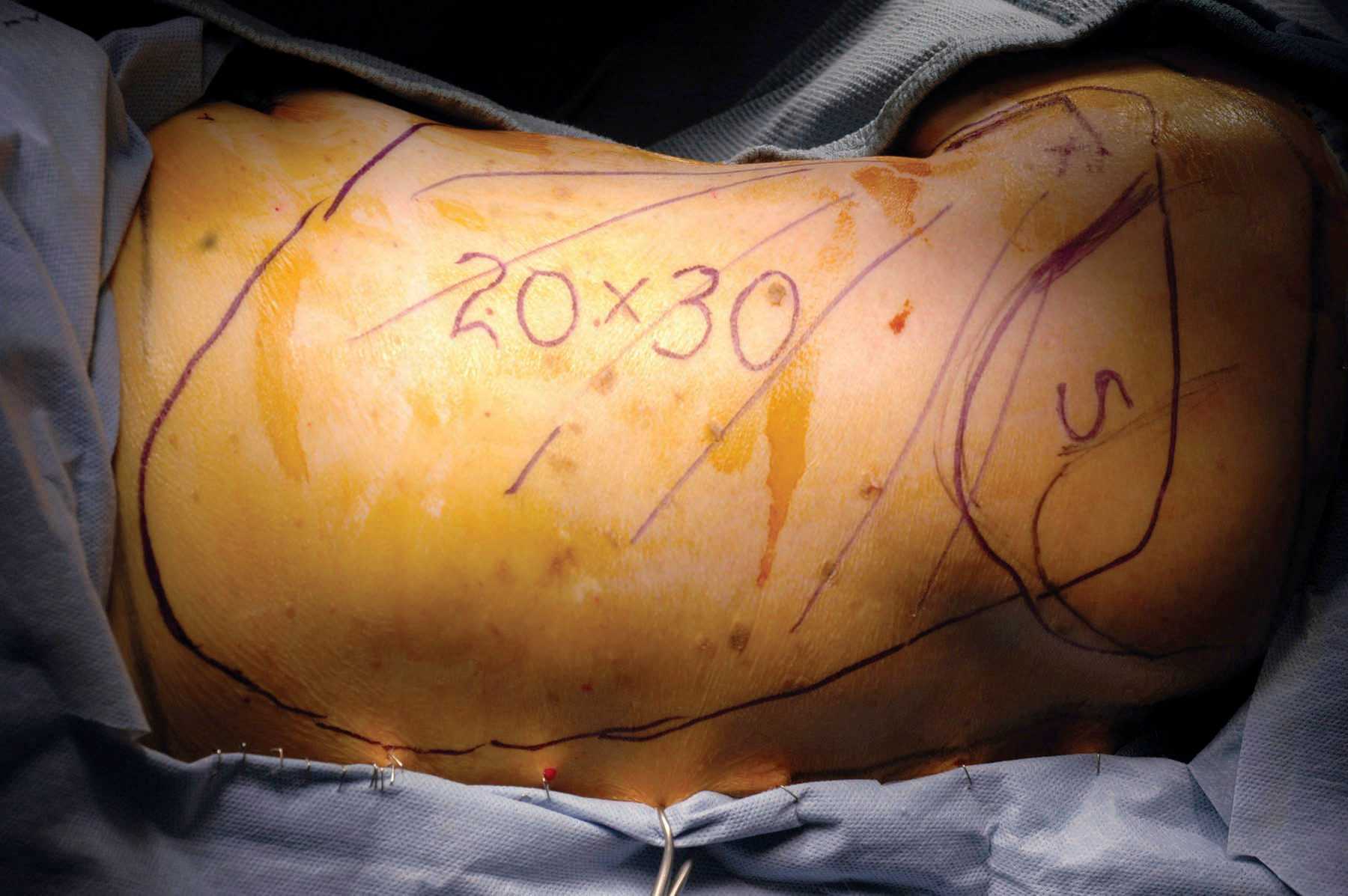
D E F
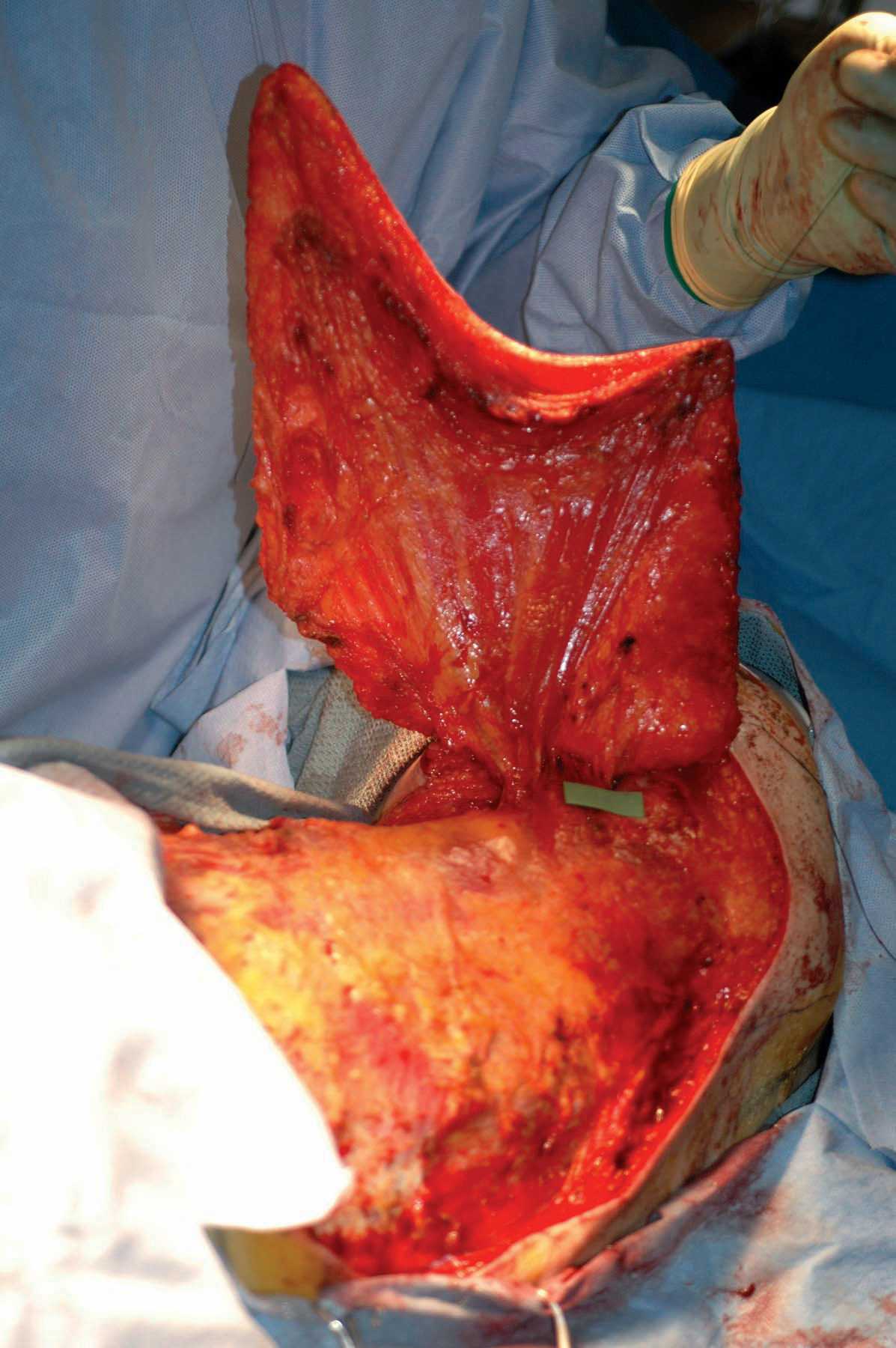
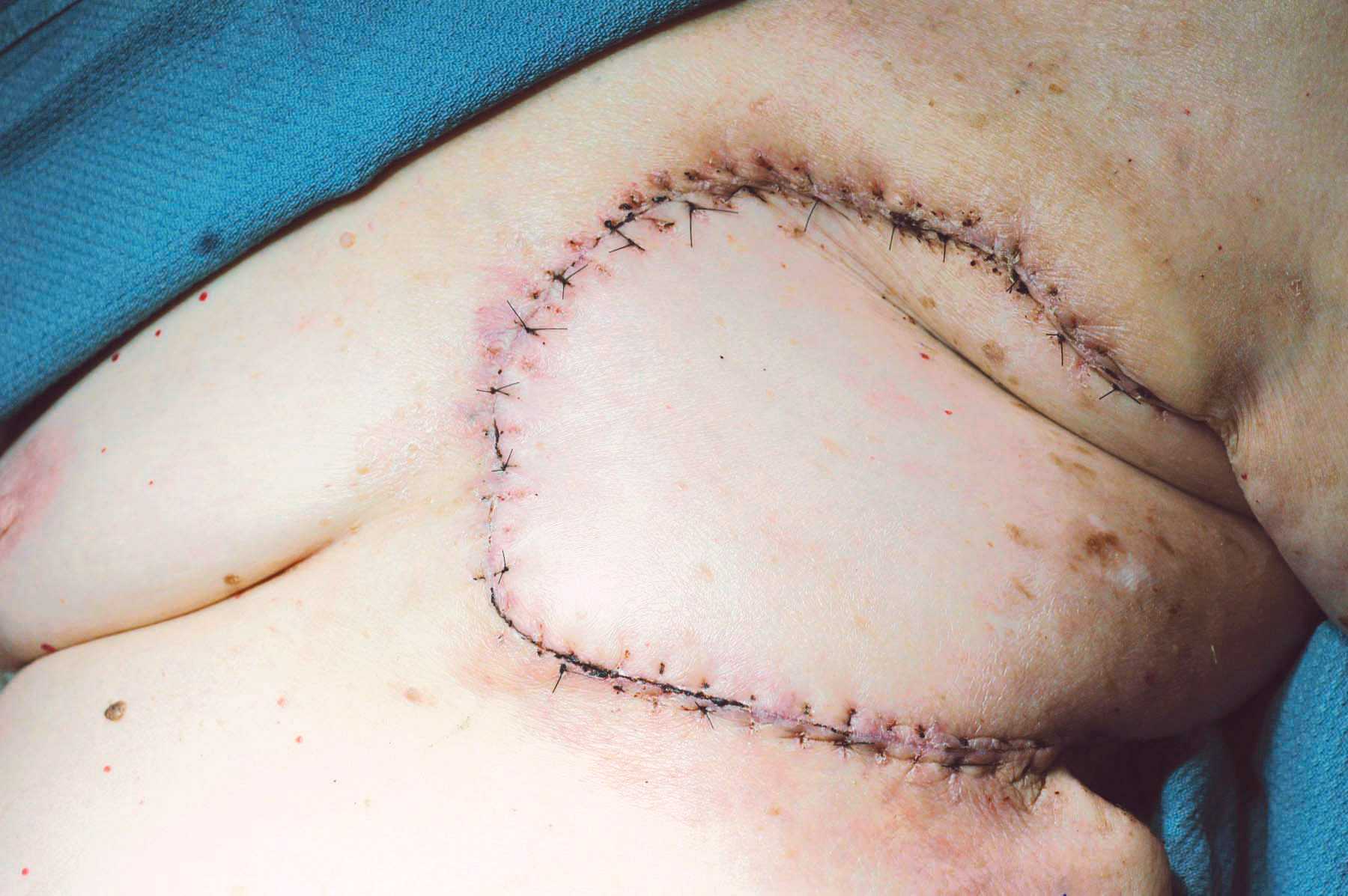
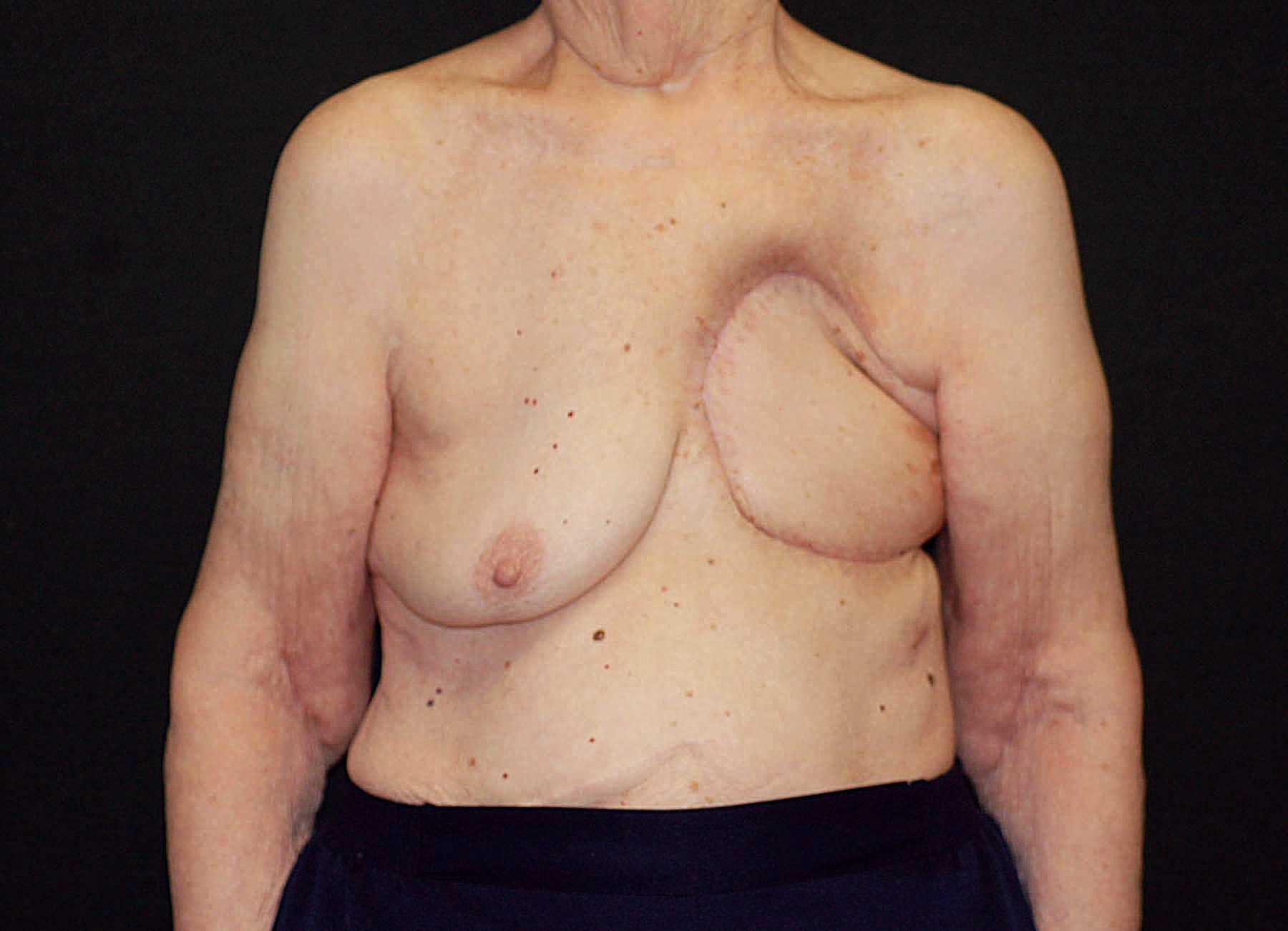
Figure 2. (A) Chronic ulcer with exposed ribs at left mastectomy site as a sequela of radiation treatment. (B) Huge defect following removal of all non-living material, with lung exposed. (C) Design of correspondingly huge LD musculocutaneous flap on left back. (D) The entire flap raised remaining attached only by its blood vessels (on the green grid) in the armpit. (E) Flap swung and then sewn in place to close the left chest hole. (F) Healed wound several months later.
Equipment
No specialized equipment other than routine surgical instruments are needed to raise an LD muscle flap.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Acknowledgments
Kate Mertz, Surgical Technician, from Bowmanstown, Pennsylvania, was the first assistant for all surgery.
Citations
- Robinson DW. Surgical problems in the excision and repair of radiated tissue. Plast Reconstr Surg. 1975;55:41-49. doi:10.1097/00006534-197501000-00007.
- Hallock GG, Morris SF. Skin grafts and local flaps. Plast Reconstr Surg. 2011;127:5e-22e. doi:10.1097/PRS.0b013e3181fad46c.
- Lee KT, Mun GH. A systematic review of functional donor-site morbidity after latissimus dorsi muscle transfer. Plast Reconstr Surg. 2014;134:303-314. doi:10.1097/PRS.0000000000000365.
- Blondeel PN. One hundred free DIEP flap breast reconstructions: a personal experience. Br J Plast Surg. 1999;52:104-111. doi:10.1054/bjps.1998.3033.
- Disa JJ, McCarthy CM, Mehrara BJ, Pusic AL, Cordeiro PG. Immediate latissimus dorsi/prosthetic breast reconstruction following salvage mastectomy after failed lumpectomy/irradiation. Plast Reconstr Surg. 2008;121:159e. doi:10.1097/01.prs.0000304235.75016.02.
- Santanelli di Pompeo F, Laporta R, Sorotos M, Pagnoni M, Falesiedi F, Longo B. Latissimus dorsi flap for total autologous immediate breast reconstruction without implants. Plast Reconstr Surg. 2014;134(6):871e-879e. doi:10.1097/PRS.0000000000000859.
- Taylor GI, Daniel RK. The free flap: composite tissue transfer by vascular anastomosis. ANZ J Surg. 1973;43:1-3. doi:10.1111/j.1445-2197.1973.tb05659.x.
- Maxwell GP. Iginio Tansini and the origin of the latissimus dorsi musculocutaneous flap. Plast Reconstr Surg. 1980;65:686-691. doi:10.1097/00006534-198005000-00027.
- Angrigiani C, Grilli D, Siebert J. Latissimus dorsi musculocutaneous flap without muscle. Plast Reconstr Surg. 1995;96:1608-1614. doi:10.1097/00006534-199512000-00014.


| Publication Date | 9/4/2024 |
| Article ID | 290.7 |
| Production ID | 0290.7 |
| Volume | 2024 |
| Issue | 290.7 |
| DOI | |
| https://doi.org/10.24296/jomi/290.7 | |