Temporal Bone Dissection (Cadaver)
Abstract
Temporal bone dissections are a critical learning tool for otologic/neurotologic surgery. The “Temporal Bone Dissection Manual" from the House Institute has long served as a ‘gold standard’ for the stepwise demonstration of this process. In this video, a progressive step-by-step dissection of the temporal bone is performed. Key anatomical structures and landmarks and outlined, and their physiological importance in the context of different otologic pathologies is explained. The procedure begins with the identification of soft tissue landmarks and surface anatomy before delving into cortical mastoidectomy and facial nerve identification. The mastoid tip region is discussed, before moving on to describe the tegmen and endolymphatic sac. A facial recess dissection is performed and middle ear anatomy is explained. A labyrinthectomy and exposure of the internal auditory canal conclude the dissection. In addition to going over the anatomy of the temporal bone dissection, a discussion of how to execute these procedures safely and efficiently is conducted.
By having a thorough understanding of the anatomy of the temporal bone, medical students, residents, and fellows are better able to understand the reasoning behind different otologic procedures and how they can be used to treat patients. This demonstration was created to inform and teach residents and medical students about temporal bone anatomy.
Keywords
Otology; neurotology; anatomy; mastoid; skull base surgery; otolaryngology; temporal bone.
Background
Temporal bone dissections are an essential learning tool prior to performing surgeries of the mastoid and lateral skull base. Accurately knowing anatomical locations of all landmarks is critical to operating in the area safely and efficiently. In addition, performing temporal bone dissections allow surgeons the opportunity to study middle ear anatomy, the otic capsule, relationships of the skull base, and other temporal bone anatomy in a way that is not possible during the normal surgical approaches, as removal/injury in the laboratory does not result in any significant consequences. From a teaching perspective, learning different surgical procedures through temporal bone dissection is a significant learning aid for students; in fact, temporal bone dissections are useful learning tools for different surgical procedures such as tympanotomy, atticotomy, mastoidectomy, cochlear implant, endolymphatic sac decompression, and facial nerve decompression.1,2
Herein we provide a step-by-step dissection of the temporal bone and the important anatomy and surgical techniques to follow when dealing with the facial anatomy are reviewed. We hope that this serves as a primary resource for temporal bone dissection or as a useful adjunct to printed temporal bone dissection manuals.
Procedural Outline
Soft Tissue Landmarks
The malar eminence, that connects posteriorly to the zygomatic arch and ultimately the root of the zygoma, is first identified. The temporal line (linea temporalis) is the posterior extension of the zygomatic root. Its relationship to underlying anatomy cannot be understated, as it is the starting point for the majority of mastoid drilling dissection. It typically approximates the junction of the mastoid cavity (inferior) and the temporal lobe of the brain (superior).
After identifying these soft tissue landmarks, a radius of 5 cm from the external auditory canal (EAC) is measured. This distance is what is used for lateral skull base approaches such as a translabyrinthine approach to vestibular schwannoma. Typical incisions for standard mastoidectomy or cochlear implant surgery are either 5 mm or 1 cm posterior to the postauricular sulcus. The importance of getting enough of the posterior fossa dura exposed behind the sigmoid sinus is emphasized. This specific approach is useful for neurosurgeons in the removal of larger tumors so that they can compress the posterior fossa dura out of the way to create greater access to the temporal area.
The location of the transverse and sigmoid junction in males and females is discussed in relation to the EAC (4 cm for females, 4.5 cm for males). This is an important landmark for the neurosurgical approach for a retrosigmoid craniotomy.
Surface Anatomy
After soft tissue landmarks are described (see Figure 1), the mastoid emissary veins are identified. These veins come out to supply the periosteum and undersurface of the muscles coming from the sigmoid sinus. The Spine of Henle is then identified, which demarcates the anterior boundary of the mastoid cortex right before it dips medially to the posterior bony ear canal. The Spine of Henle serves as a landmark for the antrum medially. The cribriform area is identified next, which lies within the MacEwen’s triangle, which serves as the true approximation of the location of the mastoid antrum medially. Clinically, this landmark is significant in someone with acute otitis media with frank mastoiditis or a purulent mastoiditis because they can develop subperiosteal abscesses, which will cause the ear to become proptotic.
This section concludes with a demonstration of surgical technique with the specific Stryker drill used in the dissection. This specific drill has 5 different length settings and a setting of 3 was used for this procedure. The importance of testing the drill pedal is underscored to ensure it’s going in the right direction, starting along the temporal line, and gripping the drill with two fingers (pointer and thumb) to make sure not to obstruct the line of sight.
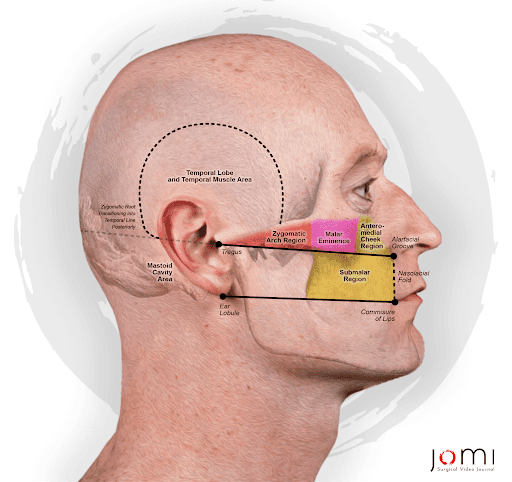
Figure 1. Soft Tissue Landmarks for Lateral Skull Base Surgery.
Cortical Mastoidectomy
Cuts begin along the temporal line and then inferiorly towards the mastoid tip along the posterior ear canal. The deepest part of the dissection should always be anterior and superior into the mastoid; this technique will help you work your way into the antrum while avoiding the brain, sigmoid sinus, and posterior fossa dura. Most sclerotic mastoids will still contain an air cell just lateral to the lateral semicircular canal (LSCC). The temporal line approximates the floor of the cranial fossa and is a good starting point for the dissection. One can observe a layer of vessels (venous plexus) within the bone overlying the temporal lobe dura. The LSCC can be found medial to the trabecular bone of the mastoid air cells. After identifying the lateral canal, the epitympanic bone can be opened between dura and superior EAC to identify the short process of the incus. The surgeon may use light refraction through water/irrigation to see the incus prior to the drill uncovering the bone immediately lateral/posterior to it.
The goal by the end of this section is to get an en face view of the posterior ear canal so that you can get a sharp and thin posterior EAC. This will also allow for the visualization of the disappearance of air cells along the posterior EAC as well as a color change when thinning the bone near the EAC skin.
Facial Nerve Identification
Identification of the facial nerve begins by having the appropriate landmarks exposed. These include the LSCC and the short process of the incus. The EAC should be adequately thinned. Bone is removed from superior-to-inferior in the direction of the expected location of the facial nerve. A cutting burr may be used close to the facial nerve, and the timeframe of switching to a diamond burr is variable and surgeon-dependent.
At the end of this section, the chorda tympani branch of the facial nerve should be visible. The branch comes off after the second genu and courses superiorly before moving anteriorly into the middle ear and over the long process of the incus.
Digastric Ridge
When neurosurgeons/ENT oncologists expose the temporal bone externally on the mastoid cortex or behind that, they use the digastric groove as landmark identification for where the muscle is attached into the bone. This is in contrast to the otologist, who identifies the digastric ridge within the temporal bone. The digastric muscle is always lateral to the facial nerve, and it can be traced posterior to anterior to safely remove the mastoid tip while protecting the facial nerve in the stylomastoid foramen.
Tegmen Exposure
This procedure is usually done with a diamond burr and involves thinning down the bone overlying the temporal lobe and deepening the sinodural angle. One point of emphasis in this section is that as you work more medially, you are confined by your dissection laterally; therefore, saucerization is critical for a surgery like a mastoidectomy so that the surgeon has a greater degree of freedom when moving their instruments, even if using them in a small area.
Endolymphatic Sac
The LSCC is one of the first landmarks during mastoidectomy surgery, and serves as an important component for locating the endolymphatic sac (ELS). Donaldson’s line is an imaginary line drawn along the LSCC from anterior to posterior, bisecting the posterior semicircular canal (PSCC), and then extending onto the posterior fossa dura anterior to the sigmoid sinus. In this area, the bone can be thinned, and depending on individual patient anatomy, decompression of the sigmoid sinus may be necessary to allow adequate access.
As the bone is thinned, an area of more thickened dura with fibers/blood vessels running in the same direction helps to better localize the ELS. The endolymphatic/vestibular aqueduct may be seen coursing toward the otic capsule, and the entrance of the duct into the petrous bone referred to as the “operculum”. The clinical correlation for the identification of the endolymphatic sac is that decompression of this structure may be used in the treatment of Meniere’s disease.
Middle Ear Anatomy
At this point, a facial recess dissection has been completed and access to the middle ear is through a posterior tympanotomy. The pyramidal process, containing the stapedius muscle, is located just medial to the facial nerve. The stapedius muscle gives rise to the stapedial tendon that is attached to the capitulum of the stapes. The stapes superstructure and footplate are identified.
After identification of the pyramidal process and stapedius muscle, the next step is to remove the incus to be able to visualize the tympanic segment of the facial nerve. After removing the incus and incus buttress, the cochleariform process and tensor tympani tendon should be visible. The head of the malleus may need to be removed to facilitate this as well.
Labyrinthectomy
While there are multiple ways to perform a labyrinthectomy, choosing a consistent and methodical technique will ensure safe and efficient surgery. I prefer starting with anterior to posterior cuts along the LSCC, while leaving the inferior bone to protect the second genu of the facial nerve. Much like tracing Donaldson’s line, this can then transition into removal of the PSCC. I start inferiorly away from the crus comminura at the ampullated end of the PSCC. Ensure on preoperative imaging that the jugular bulb does not approximate this area, which is possible in some instances. The lumen can be tracked towards the common crus and then the vestibule is opened. The superior canal lumen can then be traced, which may or may not require tegmen decompression and elevation of the temporal lobe with gentle retraction. This depends on the aeration of the temporal bone. Of note, the saccule and posterior canal are innervated by the inferior vestibular nerve, while the utricle, superior, and LSCCs are innervated by the superior vestibular nerve.
The final step in this section is to open the vestibule by thinning the bone. Once you visualize the vestibule, you can identify the spherical and elliptical recesses, which represent locations of the utricle and saccule respectively.
Internal Auditory Canal
This section begins by showing that the internal auditory canal (IAC) is completely encased within the temporal portion of the petrous bone. The ampullated end of the superior semicircular canal serves as the superior border of the IAC, while the ampullated end of the PSCC serves as the inferior border. The IAC angle is often comparable to that of the EAC, but the dissection surface moves from medial to lateral as goes from posterior to anterior.
Finally, the demonstration is concluded by describing the pathway of the facial nerve: the intrameatal/intracanalicular nerve exits through the fundus to become the labyrinthine segment of the facial nerve; this branch makes its first genu at the geniculate ganglion and becomes the tympanic segment before making its second genu into the descending/mastoid segment and exits the temporal bone through the stylomastoid foramen.
Discussion
Temporal bone dissections aid in the learning of critical anatomic landmarks and their variations when performing otologic procedures. A hands-on approach when studying anatomy is crucial for medical students and residents to understand the temporal bone anatomy. In order to overcome the challenges of temporal bone surgery, it is essential for trainees to develop hand-eye coordination and fine hand movements during the surgery and to attain anatomical knowledge under microscopic vision.3
In addition to learning temporal bone anatomy, performance of different procedures on temporal bone models can be used to assess fundamental surgical skills. Specifically, the CanadaWest scale delineated performance by experience level with strong interrater reliability and was successful in distinguishing junior from senior trainees.4 These objective scales are an important indicator of progress being made in a trainee with respect to their surgical abilities.
While using a cadaveric model for temporal bone dissection is useful, these cadavers are often hard to obtain in practice; therefore, simulators have become increasingly common to use in training residents and medical students for different otologic procedures. Despite not being as effective as learning from cadavers, simulators and the development of new teaching tools should be encouraged to continuously improve surgeon trainees.5
Ultimately, temporal bone dissections using a cadaver serve as an essential learning tool for otologic surgical trainees. This dissection can be used to teach foundational anatomy to medical students learning temporal anatomy for the first time, or to assess the surgical skills of otologic surgeons throughout their training. While cadavers have been the gold standard in performing these dissections, simulators and 3D models are also increasing in their prevalence.
Equipment
The only specialized equipment used for this dissection was a Stryker drill. Remaining instruments were standard for a typical “ear tray”, such as ear curettes, alligator forceps, microscissors, and suction tip.
Disclosures
C. Scott Brown serves as editor for the Otolaryngology section of the Journal of Medical Insight.
Citations
- Jatale SP, Chintale SG, Kirdak VR, Shaikh KA. Our experience of anatomical variations of facial nerve in cadaveric temporal bone dissection. Indian J Otolaryngol Head Neck Surg. 2021 Sep;73(3):271-275. doi:10.1007/s12070-020-01969-9.
- Prasad KC, K Prthyusha, Maruvala S, R HT, Gopi IV, R SK. Impact of temporal bone dissection on the understanding anatomy of the ear among medical students. Int J Otorhinolaryngol Head Neck Surg. 2018;4(6):1489. doi:10.18203/ISSN.2454-5929.IJOHNS20184365.
-
Irugu DV, Singh AC, Sikka K, Bhinyaram J, Sharma SC. Establishing a temporal bone laboratory in teaching institutes to train future otorhinolaryngologists and fundamentals of temporal bone laboratory: considerations and requirements. Indian J Otolaryngol Head Neck Surg. 2016 Dec;68(4):451-455. doi:10.1007/s12070-015-0962-0.
-
Pisa J, Gousseau M, Mowat S, Westerberg B, Unger B, Hochman JB. Simplified Summative Temporal Bone Dissection Scale demonstrates equivalence to existing measures. Ann Otol Rhinol Laryngol. 2018 Jan;127(1):51-58. doi:10.1177/0003489417745090.
-
Okada DM, de Sousa AM, Huertas Rde A, Suzuki FA. Surgical simulator for temporal bone dissection training. Braz J Otorhinolaryngol. 2010 Sep-Oct;76(5):575-8. doi:10.1590/S1808-86942010000500007.

| Publication Date | 8/23/2024 |
| Article ID | 314 |
| Production ID | 0314 |
| Volume | 2024 |
| Issue | 314 |
| DOI | |
| https://doi.org/10.24296/jomi/314 | |