Neuronavigation and Endoscopy as Adjunctive Tools in Orbital Floor Implant Revision: Surgical Management of Infected, Misplaced Orbital Floor Implant with Chronic Eyelid Fistula and Sinusitis
Abstract
Orbital floor fractures represent common sequelae of facial trauma that may result in significant functional and aesthetic consequences. This article presents a comprehensive overview of the management of a revision case involving an orbital floor fracture, focusing on complications related to extruded, infected orbital hardware. In addition, common mistakes that involve improper placement of orbital floor implant, poor implant sizing, and lack of adequate implant fixation are discussed.
The featured case involves delayed wound healing and a sino-orbital cutaneous fistula (SOCF) due to infected orbital hardware from a previous orbital floor fracture repair. The discussion centers on preoperative planning, including the choice of surgical approach (transconjunctival with lateral canthotomy) and implant material. Intraoperative neuronavigation was utilized as an adjunctive tool to confirm the position of the newly placed orbital implant. This case provides valuable insight on preventable complications for this procedure, nuances in surgical approach, and uncommon challenges faced by providers who perform operative facial trauma repair.
Keywords
Orbital fracture; orbital floor; transconjunctival approach; hardware infection; orbital implant; Medpor; polyethylene; titanium; eyelid fistula.
Case Overview
Background
Pneumo-orbit, involving air in the orbital cavity, often stems from sinus-to-orbit connections after orbital trauma. While such cases typically heal spontaneously postfracture repair, persistent fistulas indicate underlying issues. Case reports highlight sino-orbital cutaneous fistula (SOCF) from non-autologous orbital trauma implants.1–3 In this case, hardware misplacement into the maxillary osteomeatal complex led to ongoing sinus obstruction, creating an anomalous passage to the lower eyelid skin weakened by infected hardware. Addressing this challenging scenario is crucial for restoring normal bony anatomy and preventing similar complications in the future.
History of the Patient
A 34-year-old male initially sought care for chronic recurrent drainage under his right eye, stemming from a right orbital blowout fracture seven years ago due to assault. The fracture was initially repaired with open reduction and internal fixation at another institution. Since then, he has experienced intermittent purulent drainage from the right nasal cavity and a lower eyelid fistula. He also noted air movement through the prior incision site when blowing his nose and delayed-onset diplopia with enophthalmos. After initial surgery, the patient underwent multiple courses of antibiotics with waxing and waning symptom improvement.
Physical Exam
The physical exam revealed a 3-cm skin dehiscence at the infraorbital rim with crusting and purulent drainage upon palpation. Mild erythema was noted along the skin of the right infraorbital rim at the fistula site. The patient reported mildly decreased right V2 sensation. Diplopia was observed in both primary and directional gazes, and extraocular movements were intact with preserved visual acuity. Nasal endoscopy revealed purulent drainage from the right middle meatus.
Imaging
Computed tomography (CT) maxillofacial imaging revealed displaced prior hardware along the right orbital floor (Figure 1–3). The right maxillary sinus exhibited complete opacification, indicating presumed chronic maxillary sinusitis and osteomeatal complex obstruction. Persistent bony defects were noted in the medial orbital wall and orbital floor. In sagittal view, the implant was displaced into the maxillary sinus, failing to reconstruct the posterior orbital floor defect. Axial view showed the orbital floor implant extending beyond the infraorbital rim, with an air pocket around a screw, suggesting hardware failure with infection.
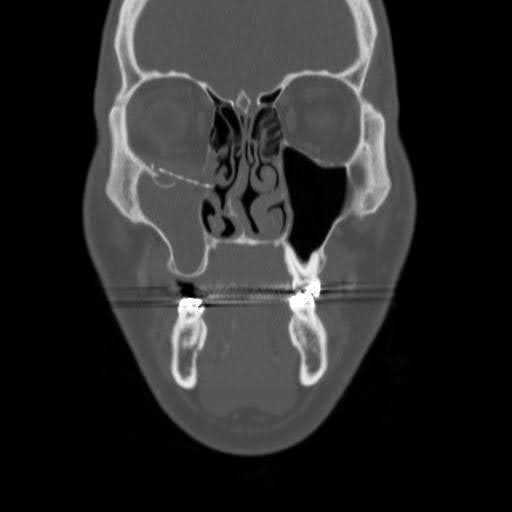
Figure 1. Preoperative non-contrast coronal CT scan. CT image demonstrating inferior displacement of the medial aspect of the orbital floor implant and the connection between the paranasal sinuses and orbital cavity.

Figure 2. Preoperative non-contrast sagittal CT scan. CT image demonstrating inferior displacement of the orbital floor implant into the maxillary sinus as well as inadequate posterior seating on the residual orbital floor.

Figure 3. Preoperative non-contrast axial CT scan. CT image demonstrating free air adjacent to the lateral screw in the orbital rim.
Workup
Orbital trauma workup necessitates a thorough physical examination focusing on external deformities, along with a comprehensive ophthalmic and neurologic examination. Preoperative imaging with fine-cut non-contrast CT scans aid in intraoperative decision-making. When integrated with neuronavigation, CT assists in differentiating landmarks, particularly in distorted anatomy.
Rationale for Treatment
The foremost priority was eliminating the source of ongoing infection by removing compromised hardware. Next, addressing persistent diplopia by restoring premorbid orbital volume was crucial. The third priority focused on resolving the blockage of the maxillary sinus drainage pathway leading to persistent maxillary sinusitis. The final goal encompassed addressing the eyelid scar resulting from the fistula and improving cosmesis.
Special Considerations
Patients presenting with hardware infections beyond one month postoperatively, especially those who have failed multiple antibiotic courses, typically benefit from complete hardware removal due to potential biofilm formation.4 Surgical intervention is often recommended for patients with persistent diplopia and globe malpositioning lasting more than 1–3 months, as advised by senior authors (TL, DS).
Revision orbital surgery may not be necessary if hardware infection responds to antibiotics within the first month postsurgery, prior to biofilm formation. In cases of severe orbital trauma, such as intraconal hemorrhage or retinal detachment, surgery is contraindicated to minimize the risk of further intraoperative orbital injury from globe retraction.
Surgical Details
The patient in this case underwent 1) orbital hardware removal with a postseptal, transconjunctival approach and lateral canthotomy, 2) orbital floor implant replacement using a Medpor-titanium implant with neuronavigation, 3) conservative maxillary antrostomy with tissue removal, and 4) eyelid fistula excision with local tissue advancement closure.
The patient’s facial region was draped with the contralateral orbit exposed to assess for symmetry. Lidocaine and epinephrine were injected for hemostasis and hydrodissection of tissue planes, particularly at the orbital rim where tethering around the fistula had occurred. The senior author (TL), as a matter of preference, operates with a corneal shield. Subsequently, a lateral canthotomy was performed to enhance exposure and mobilize the lower lid.
Orbital floor fractures are generally approached through transconjunctival or transcutaneous approaches. Transcutaneous incisions, such as the subciliary, subtarsal, and orbital rim approaches, pose a higher risk of postoperative ectropion.5–8 In contrast, the transconjunctival approach is preferred due to its avoidance of external incisions, resulting in lower rates of ectropion or retraction, while preserving the innervation of the orbicularis muscle.9, 10
The senior authors (TL, DS) favor a transconjunctival incision in a postseptal plane down to the orbital rim. Although this dissection plane is considered simpler, there is no statistically significant difference in rates of entropion, ectropion, foreign body sensation, and scar formation.9 In the transconjunctival approach, preserving the tarsal plate is crucial. The incision should be made near the infraorbital rim, with the lower eyelid retracted using a Desmarres retractor. If the incision is medial to the punctum, caution is needed to prevent injury to the canaliculus and lacrimal system. Staying close to the caruncle or transitioning to a transcaruncular incision can help mitigate the risk of damage.
In this case, identifying the subperiosteal tissue plane through the transconjunctival incision was difficult due to fibrosis and adhesions from the previous infection along the infraorbital rim. To address this, the lateral canthotomy site was used to initially identify the subperiosteal tissue plane along the lateral orbital wall, which was then carried centrally to the transconjunctival incision. Deeper in the postseptal plane, the Jaeger lid and malleable retractors facilitated the retraction of orbital fat posteriorly during dissection down to the infraorbital rim. The orbital floor implant was discovered within the maxillary sinus, and a #9 periosteal elevator was used to lift the orbital contents by dissecting immediately superficial to the displaced implant. This maneuver allowed a malleable to sweep the herniated orbital content superiorly while identifying stable peripheral orbital bone. Debridement of bony fragments from the maxillary sinus was performed with care to preserve the infraorbital nerve and extraocular muscles.
Nasal endoscopy revealed hardware extrusion medially beneath the uncinate process, forming an abnormal fistula connecting nasal, maxillary sinus, and orbital cavities. Consideration of ipsilateral maxillary mega-antrostomy was debated but was deferred due to the concerns about increased orbit-nasal communication and implant exposure. Instead, a conservative maxillary sinusotomy was performed by extending the natural maxillary sinus opening inferiorly to prevent recirculation with plans for serial CT imaging for potential future definitive sinus surgery if sinusitis recurs.
Following removal of the previous implant, significant herniation of orbital content into the sinus from the orbital floor and medial orbital wall defect was noted. A new orbital floor implant was placed, stabilized by identifying solid posterior and medial bony ledges with neuronavigation.
A polyethylene-coated (Medpor) titanium implant was chosen to avoid periorbital scar contracture associated with bare titanium. The implant was soaked in Betadine, contoured to fit the natural orbit curvature, and trimmed for stability without extending beyond the infraorbital rim. Neuronavigation in the coronal view ensured proper positioning. Screws and the implant were placed behind the infraorbital rim, with one screw typically sufficient, anchored through the orbital floor implant. Due to near total orbital floor defect, a prong extending from the implant was used to secure the implant. In cases of inadequate stable orbital floor, screws should be placed in regions with thicker skin, such as along the nasal sidewall or lateral orbital rim. Nasal endoscopy post-reimplantation confirmed proper positioning, resolving the initial medial displacement blocking the maxillary sinus drainage pathway.
Before closure, the cutaneous eyelid fistula borders were excised, and local tissue advancement lifted the eyelid scar contracture off the infraorbital rim. The lateral canthal tendon was reapproximated onto the Whitnall’s tubercle with 4-0 clear nylon.
To reduce entropion risk, absorbable suture (5-0 fast absorbable gut in this case) was used by the senior author (TL) for transconjunctival incision closure, which is a matter of surgeon preference.
Postoperative Care
The patient was observed overnight and discharged the next day. Immediate postoperative CT imaging (Figures 4–6) confirmed proper orbital hardware positioning. Sinus precautions (avoiding nose blowing, bearing down, or increasing intrathoracic pressure) were advised to prevent potential vascular and visual compromise due to unintentionally trapped orbital air, and Augmentin was prescribed for 7 days. Due to the pre-existing nasal-orbital fistula, sinus irrigations were deferred.
At the 8-month follow-up, the patient reported significant diplopia improvement, with intact extraocular movements and no recurrence of eyelid fistula or sinusitis. Clinical progress will be monitored with serial CT sinus imaging for potential maxillary sinusitis recurrence.
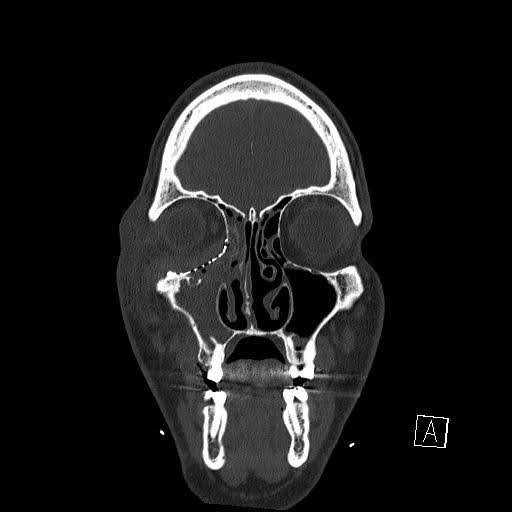
Figure 4. Immediate postoperative day 1 coronal non-contrast CT scan. CT image demonstrating the presence of early persistent opacification in the right maxillary sinus.

Figure 5. Immediate postoperative day 1 axial non-contrast CT scan. CT image demonstrating the new orbital floor implant, which does not extend beyond the infraorbital rim.

Figure 6. Immediate postoperative day 1 sagittal non-contrast CT scan. CT image demonstrating appropriate orbital floor implant positioning with the posterior portion resting above a stable ledge of posterior orbital bone.
Discussion
This case presented a delayed SOCF resulting from hardware malpositioning, requiring removal of infected hardware, restoration of native anatomy, and correction of diplopia.
Surgical indications for orbital floor repair include: 1) extraocular muscle entrapment with or without oculocardiac reflex, 2) malpositioned globe with persistent diplopia, 3) diplopia with an orbital defect (larger than 2–3 cm2 with at least 3 mm of displacement) and resulting enophthalmos or a fracture involving over 50% of the orbital floor, 4) extruded or infected orbital hardware, and 5) a persistent SOCF that does not resolve with conservative management.11–15
Late complications of orbital surgery, arising from delayed wound healing, fibrosis, and scar contracture, encompass a spectrum of issues often requiring revision surgery. These complications include ectropion, entropion, hardware failure, chronic infections, fistula formation, persistent paresthesias, and lagophthalmos. Scar contracture and lamellar shortening from various surgical approaches can lead to ectropion and entropion.16 The transconjunctival approach, preserving the tarsus, is preferred for patients with a negative vector, reducing the risk of ectropion formation.
Persistent diplopia, occurring in 8–52% of cases for weeks postoperatively, is exacerbated by preoperative edema, intrinsic fibrosis, muscular ischemia, inflammation, and improper implant placement causing extraocular muscle impingement.5,7,17 Imaging aids in identifying causes of diplopia. If postoperative orbital volume is normal, observation allows for potential central nervous system compensation. In this case, persistent diplopia resulted from improper implant placement, shape, and size, causing inadequate orbital volume. Distinct from globe malpositioning, traumatic injuries to cranial nerves or extraocular muscles can also cause prolonged diplopia with strabismus. After restoring proper orbital volume and globe position, a strabismus specialist is essential for assessing and treating diplopia from these injuries.
Another late complication includes delayed enophthalmos (occurring in 7–27% of cases postoperatively) and hypoglobus, which can gradually emerge due to tissue deficits from prior devascularization and ischemia.5,12,18 However, a more common cause, as observed in this case, is the aberrant expansion of the orbital cavity with implant displacement or improper sizing. Effectively addressing late enophthalmos poses challenges and may necessitate implant replacement or augmentation to restore proper orbital volume.5
Recent studies emphasize the advantages of individualized implants created through selective 3D printing with improved outcomes and lower revision rates comparable to intraoperative neuronavigation.19,20 Drawbacks include increased cost and manufacturing delays of a few weeks.20 The decision between individualized and non-individualized implants should be tailored. The senior author (TL) typically reserves customized orbital floor implants for patients with complex zygomaticomaxillary fractures and concurrent orbital floor fractures requiring simultaneous correction of malar flattening.
To prevent orbital complications, it's crucial to avoid common mistakes during the initial surgery. We will briefly describe potential factors that may have contributed to the complications seen in this patient. Inadequate exposure may have played a significant role for this patient. The orbital implant should ideally rest on the stable posterior and/or lateral orbital floor and a stable medial orbital wall. Our patient's significant medial orbital wall defect, extending posteriorly, was likely not properly exposed. In cases like this, a transcaruncular incision posterior to the nasolacrimal duct, in addition to a transconjunctival approach, may be necessary for proper medial orbital wall exposure. Cautious subperiosteal dissection minimizes injury during superior dissection along the medial orbital wall, where identifying arteries like the anterior ethmoidal and posterior ethmoidal is crucial. Staying in the subperiosteal plane is also key to preserving structures like the inferior oblique muscle during intraorbital dissection.
Similarly, the fracture extends quite extensively posteriorly along the orbital floor, and this region likely remained inadequately exposed. This is evident from the inferior displacement of the implant into the maxillary sinus. Given the presence of crucial cranial nerves and extraocular muscles at the orbital apex, there is a natural hesitation and anxiety associated with dissecting in this area. The use of neuronavigation, particularly in revision cases, adds an additional layer of reassurance and certainty, especially when dealing with significantly altered anatomy. Insufficient exposure of the fracture leads to incomplete reduction and potential complications, including implants displacing into the sinus, resulting in globe malposition or the entrapment of orbital tissue. This, in turn, can lead to limitations in extraocular motility due to the tethering of the extraocular muscles.
When designing the implant shape, it is important to be mindful of the gentle S-curve of the natural orbital floor when viewed in a sagittal plane. The floor descends immediately posterior to the rim and then gently climbs upwards closer to the orbital apex. Along the medial orbital floor, there is a gentle transition to the medial orbital wall. Unfortunately, it appears that the original orbital floor implant did not follow these contours, resulting in reconstruction of a portion of the orbital floor defect without the medial orbital wall component. This likely further contributed to chronic sinusitis and eyelid fistula formation after the medial component of the orbital implant obstructed the natural osteomeatal complex that allows for proper maxillary sinus drainage. Once chronic sinusitis developed, bacterial colonization developed along the orbital aspect of the implant and further contributed to ongoing periorbital infection.
Regarding implant sizing, it is important to shape it so that the implant sits posterior to the infraorbital rim to prevent erosion of the hardware through the lower eyelid. It is best to avoid excess hardware placement along the anterior surface of the infraorbital rim to prevent implant palpability, undesirable scarring, and/or hardware exposure as seen in this particular patient. In respect to anterior and posterior dimensions of the orbital floor implant, the implant should be sufficiently long enough to reach stable bone located posteriorly while being careful to avoid impinging the orbital apex contents. During the implant sizing and shaping process, neuronavigation can help identify stable medial, posterior, and lateral orbital bone for implantation. After placement of a new orbital floor implant, a neuronavigation probe can be used to trace the outline of the new orbital floor hardware to ensure proper shape, positioning, and stability intraoperatively. The intraoperative usage of neuronavigation may be of particular benefit in a complex orbital revision case such as this or in patients with concurrent sinus or skull base issues.
A costlier option is intraoperative CT scanning, where the orbital floor implant is placed and scanned to confirm implant positioning. This allows for immediate adjustments without the need for additional trips to the operating room. It's important to note that despite many studies comparing surgical outcomes to the contralateral eye, there may not always be an exact 3D symmetry in both orbits.21
To prevent delayed hardware migration, fixation of the orbital floor implant is crucial. Ideally, the fixation screw should pass through the implant, securing it to a stable segment of the orbital floor. In cases with a near-total orbital floor defect, hardware can be secured to stable bone along the infraorbital rim. Optimal screw placement is along the medial or lateral extremes of the orbit, where the overlying skin is thicker (nasal skin or lateral canthal regions). In this case, the original hardware's excess titanium was placed along the central segment of the infraorbital rim that underlies thin lower eyelid skin, contributing to the hardware failure issue.
The senior authors (TL, DS) recommend porous polyethylene (Medpor) or Medpor-titanium hybrid implants to minimize abnormal scarring, soft tissue ingrowth, and scar contracture. Medpor-titanium implants have radiopacity for easy identification on CT scans, unlike radiolucent Medpor alone. Studies consistently show lower rates of orbital adherence syndrome with Medpor implants compared to bare titanium plates.22–25 The polyethylene coating promotes fibrovascular ingrowth without cicatricial tethering, crucial in revision cases for diplopia.17,23
After removing the original hardware in the case of persistent infection, the decision to place another orbital floor implant depends on the ability to maintain globe position. In this patient, severe hypoglobus and enophthalmos were anticipated due to increased orbital volume and lack of support along the orbital floor and medial wall. Given there was no gross purulent infection and there was healthy surrounding tissue, an immediate alloplastic orbital floor reconstruction was performed. In cases of active infection, debridement and the use of vascularized autogenous grafting material may be considered. One option that has been successfully employed by the senior author (TL) is an iliac bone graft wrapped in a vascularized pericranial flap from the cranial vault (Figure 7). If there is any potential of sinonasal contamination or lingering infection, wrapping the entire bone graft with a pericranial flap is essential to avoid total bone graft failure.

Figure 7. Iliac bone graft used to reconstruct medial and orbital floor defect. This is an intraoperative photograph of an iliac bone graft (left and central) wrapped in a vascularized pericranial flap from the cranial vault; it can be used to reconstruct the orbital floor (right). This particular patient had an infected orbital floor implant with a previous history of radiation. Due to concerns of radiated skin not tolerating Medpor orbital implant, the patient’s orbit was reconstructed with iliac bone graft. This type of non-vascularized bone reconstruction should be wrapped in vascularized pericranial flap if there is any potential for sinonasal communication or infection.
In conclusion, revision orbital floor fracture cases can present with a unique set of complications that require multiple factors to be considered for successful treatment. Using a combination of adjunctive tools such as intraoperative neuronavigation and nasal endoscopy may be helpful in managing a complex orbital fracture case with concurrent sinusitis. Careful consideration for surgical approach and orbital hardware material may also contribute to the long-term success of the surgery.
Equipment
- Medtronic StealthStation Neuronavigation.
- Stryker Medpor-Titanium Orbital implant.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Anabtawi M, Tompkins H, Salvi SM, Lee NJ. Management of recurrent pneumo-orbit secondary to post traumatic sino-orbital fistula using a navigation-guided customised 3D printed titanium implant: a case report and review of literature. Oral Surgery. 2021;14(3):285-294. doi:10.1111/ors.12577.
- Huelse R, Freuschle A, Hörmann K, Stuck BA. [Orbitocutaneous fistula after orbital reconstruction]. HNO. 2013;61(4):344-346. doi:10.1007/s00106-012-2529-7.
- Kim JI, Cheon TU, Kim TK, Nam JG. Sino-cutaneous fistula after using Medpor implant in orbital blowout fracture. J Craniofac Surg. 2020;31(6):1766-1767. doi:10.1097/SCS.0000000000006549.
- Lee TS, Appelbaum EN, Sheen D, Han R, Wie B. Esophageal perforation due to anterior cervical spine hardware placement: case series. Int J Otolaryngol. 2019;2019:7682654. doi:10.1155/2019/7682654.
- Boyette JR, Pemberton JD, Bonilla-Velez J. Management of orbital fractures: challenges and solutions. Clin Ophthalmol. 2015;9:2127-2137. doi:10.2147/OPTH.S80463.
- Ridgway EB, Chen C, Colakoglu S, Gautam S, Lee BT. The incidence of lower eyelid malposition after facial fracture repair: a retrospective study and meta-analysis comparing subtarsal, subciliary, and transconjunctival incisions. Plast Reconstr Surg. 2009;124(5):1578-1586. doi:10.1097/PRS.0b013e3181babb3d.
- Roth FS, Koshy JC, Goldberg JS, Soparkar CNS. Pearls of orbital trauma management. Semin Plast Surg. 2010;24(4):398-410. doi:10.1055/s-0030-1269769.
- Shin JW, Lim JS, Yoo G, Byeon JH. An analysis of pure blowout fractures and associated ocular symptoms. J Craniofac Surg. 2013;24(3):703-707. doi:10.1097/SCS.0b013e31829026ca.
- Barcic S, Blumer M, Essig H, et al. Comparison of preseptal and retroseptal transconjunctival approaches in patients with isolated fractures of the orbital floor. J Craniomaxillofac Surg. 2018;46(3):388-390. doi:10.1016/j.jcms.2017.12.013.
- Korchia D, Braccini F, Paris J, Thomassin J. Transconjunctival approach in lower eyelid blepharoplasty. Can J Plast Surg. 2003;11(3):166-170. doi:10.1177/229255030301100311.
- Bonsembiante A, Valente L, Ciorba A, Galiè M, Pelucchi S. Transnasal endoscopic approach for the treatment of medial orbital wall fractures. Ann Maxillofac Surg. 2019;9(2):411-414. doi:10.4103/ams.ams_173_19.
- Clauser L, Galiè M, Pagliaro F, Tieghi R. Posttraumatic enophthalmos: etiology, principles of reconstruction, and correction. J Craniofac Surg. 2008;19(2):351-359. doi:10.1097/SCS.0b013e3180534361.
- de Silva DJ, Rose GE. Orbital blowout fractures and race. Ophthalmology. 2011;118(8):1677-1680. doi:10.1016/j.ophtha.2011.05.001.
- Kunz C, Sigron GR, Jaquiéry C. Functional outcome after non-surgical management of orbital fractures--the bias of decision-making according to size of defect: critical review of 48 patients. Br J Oral Maxillofac Surg. 2013;51(6):486-492. doi:10.1016/j.bjoms.2012.09.016.
- Sung YS, Chung CM, Hong IP. The correlation between the degree of enophthalmos and the extent of fracture in medial orbital wall fracture left untreated for over six months: a retrospective analysis of 81 cases at a single institution. Arch Plast Surg. 2013;40(4):335-340. doi:10.5999/aps.2013.40.4.335.
- Kesselring AG, Promes P, Strabbing EM, van der Wal KGH, Koudstaal MJ. Lower eyelid malposition following orbital fracture surgery: a retrospective analysis based on 198 surgeries. Craniomaxillofac Trauma Reconstr. 2016;9(2):109-112. doi:10.1055/s-0035-1567813.
- Balaji SM. Residual diplopia in treated orbital bone fractures. Ann Maxillofac Surg. 2013;3(1):40-45. doi:10.4103/2231-0746.110078.
- Chen CT, Huang F, Chen YR. Management of posttraumatic enophthalmos. Chang Gung Med J. 2006;29(3):251-261.
- Tavassol F, Gellrich NC. [Competence and communication in the implementation of computer-assisted surgical planning]. Chirurg. 2021;92(3):194-199. doi:10.1007/s00104-020-01348-8.
- Zimmerer RM, Ellis E, Aniceto GS, et al. A prospective multicenter study to compare the precision of posttraumatic internal orbital reconstruction with standard preformed and individualized orbital implants. J Craniomaxillofac Surg. 2016;44(9):1485-1497. doi:10.1016/j.jcms.2016.07.014.
- Felding UNA. Blowout fractures - clinic, imaging and applied anatomy of the orbit. Dan Med J. 2018;65(3).
- Lee GHP, Ho SYM. Orbital adherence syndrome following the use of titanium precontoured orbital mesh for the reconstruction of posttraumatic orbital floor defects. Craniomaxillofac Trauma Reconstr. 2017;10(1):77-83. doi:10.1055/s-0036-1584398.
- Blessing NW, Rong AJ, Tse BC, Erickson BP, Lee BW, Johnson TE. Orbital bony reconstruction with presized and precontoured porous polyethylene-titanium implants. Ophthalmic Plast Reconstr Surg. 2021 May-Jun 01;37(3):284-289. doi:10.1097/IOP.0000000000001829.
- Lee HBH, Nunery WR. Orbital adherence syndrome secondary to titanium implant material. Ophthalmic Plast Reconstr Surg. 2009;25(1):33-36. doi:10.1097/IOP.0b013e3181929b6e.
- Sleem H, Wahdan W. Orbital adherence syndrome: clinical characterization and risk factor tracing (retrospective clinical research). Egyptian J Oral and Maxillofacial Surg. 2018;9:17-21. doi:10.21608/OMX.2018.5622.





| Publication Date | 1/10/2024 |
| Article ID | 410 |
| Production ID | 0410 |
| Volume | 2024 |
| Issue | 410 |
| DOI | |
| https://doi.org/10.24296/jomi/410 | |