Open Reduction and Internal Fixation of Mandibular Body and Parasymphyseal Fractures with Maxillomandibular Fixation and Broken Tooth Extraction
Abstract
This is a case discussing a 21-year-old male who suffered from both non-comminuted mandibular parasymphyseal and body fractures as a result of a motor vehicle accident, requiring open reduction internal fixation (ORIF) without postoperative maxillomandibular fixation (MMF). The fracture was complicated by a broken tooth root, which required extraction. After intraoperative MMF, ORIF was performed. The parasymphyseal fracture was plated using two locking four-hole 2-mm thick miniplates utilizing two locking screws on either side of the fracture with one plate along the alveolar surface (monocortical screw) and one along the basal surface (bicortical screw). For the right body fracture, a three-dimensional locking ladder plate was used via a transbuccal trocar approach for additional exposure needed for proper screw placement. Once the hardware was secured, the patient was taken out of MMF and restoration of premorbid occlusion was confirmed. Lastly, watertight mucosal closure was performed using absorbable sutures and Dermabond (cyanoacrylate adhesive).
Keywords
Mandible fracture; parasymphysis; symphysis, body; biomechanics; torsional; tension; compression, miniplate, lag screw, maxillomandibular fixation, MMF, intermaxillary fixation, IMF.
Case Overview
Background
Fractures of the symphysis and parasymphysis comprise about 15–29% of mandibular fractures.1, 2 Mandibular body fractures generally comprise about 11–36% of all fractures. Generally, assault or motor vehicle accidents (MVAs) are the most common causes of both fracture types.3, 4 These fractures comprise a large majority of mandibular fracture cases, and this article serves to present up-to-date management strategies.
Focused History of the Patient
This patient was a 21-year-old male who suffered an open, displaced, and non-comminuted left parasymphyseal fracture and a closed, displaced, and non-comminuted right body fracture after MVA (Figure 1). The patient had a BMI 21, ASA 2, and no previous surgeries. Other injuries included a lumbar transverse process fracture, right pneumothorax with right rib fracture, and pulmonary contusions.
Physical Exam
On exam, the patient was found to have an open bite deformity with trismus. There was an open gingival laceration over the left parasymphysis fracture. The patient also had posttraumatic hypoesthesia over the V3 distribution on the left side. Teeth numbers 9, 10, 21, and 22 were missing or broken.
Imaging
Non-contrast CT maxillofacial scan with a three-dimensional reconstruction showed a left-sided parasymphyseal fracture and right-sided body fracture along with a left cuspid mandibular tooth (tooth #22) with a fractured root (Figure 1). Postoperative CT scans, as in this case, can confirm proper reduction and fixation (Figure 2).
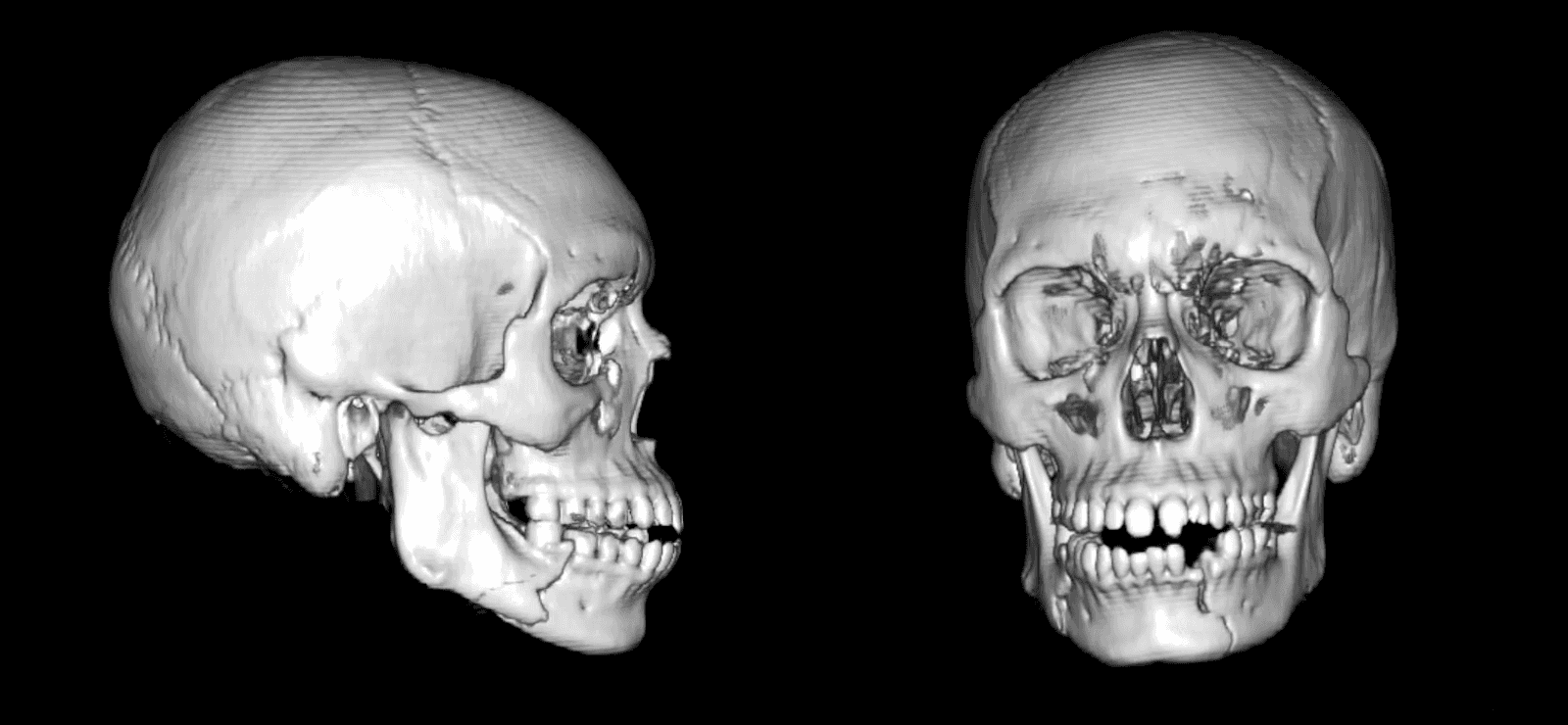 Figure 1. Preoperative CT. Scans demonstrating the displaced and non-comminuted right body and displaced and non-comminuted left parasymphyseal fractures.
Figure 1. Preoperative CT. Scans demonstrating the displaced and non-comminuted right body and displaced and non-comminuted left parasymphyseal fractures.
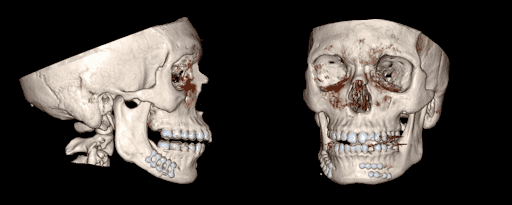 Figure 2. Postoperative CT. Scans demonstrating near anatomic bone reduction after ORIF of right body and left parasymphysieal fractures.
Figure 2. Postoperative CT. Scans demonstrating near anatomic bone reduction after ORIF of right body and left parasymphysieal fractures.
Options for Treatment
For both parasymphyseal and body fractures, open reduction and internal fixation (ORIF) is typically performed. Rarely, closed reduction may be considered with non-rigid maxillomandibular fixation (MMF) alone if there are non-displaced favorable fractures in patients who have adequate occlusion and healthy dentition.5, 6 The major disadvantage of prolonged MMF include patient discomfort, increased risk of temporomandibular joint ankylosis, inability to maintain adequate oral hygiene, and potential for airway compromise. In summary, ORIF with or without postoperative MMF offers the most reliable restoration of premorbid occlusion, bony union, and return to early function.
Rationale for Treatment
Treatment goals include 1) achieving bony union at fractures sites and 2) restoring premorbid occlusion. Nonunion can lead to chronic osteomyelitis and various infectious complications. Malocclusion can lead to patient discomfort as well as difficulty in mastication depending on the severity.
Operative Course
The patient underwent 1) intraoperative MMF, 2) dental extraction of tooth #22, 3) ORIF of both parasymphyseal and body fractures. The operative time was 1.5 hours with 110 mL of blood loss. The patient had an unremarkable postoperative course and was discharged the following day. Immediate postoperative CT scan revealed near anatomic bone reduction with adequate hardware placement, with a small fragment of retained tooth root (Figure 2). At 8 months postoperatively, the patient is currently doing well with return of normal occlusion without sign of hardware failure or infection. His preoperative V3 paresthesia resolved with the return of normal sensation. The future plan involves consideration for extraction of the remaining tooth root in a staged fashion.
Surgical Steps
In general, repair within 2 weeks is optimal if there are no other life-threatening injuries that require prioritization. Early surgery prevents the formation of tissue edema, granulation, bony calluses, or malunion. Opting for outpatient surgery with interval follow-up can help avoid unnecessary prolonged hospital stays, but there is no strong data to suggest that a delayed repair increases complication rates. However, it is worth noting that delayed repair may lead to more technical challenges, as indicated by prolonged surgical times in certain studies.7–10 It is best to avoid delaying repair beyond 2 weeks due to early bony union between displaced segments. Removal of newly formed callus and granulation between displaced fracture sites can increase surgical difficulty. Sometimes, osteotomies are performed to remove segments of bony union with gross bony displacement resulting in malocclusion.
Prior to the case, surgical airway management should be discussed with the anesthesia team.
For patients who have sustained isolated mandible fractures, the airway is secured via the nasotracheal route to allow for restoration of premorbid occlusion with intraoperative MMF and intraoral manipulation. In patients with concurrent midface or LeFort fractures with medial buttress fractures that may require rigid fixation, one may consider submental intubation or tracheostomy for airway control. Submental intubation offers superior cosmesis in young patients by avoiding a tracheostomy scar and potentially a prolonged intensive care unit stay (Figure 3). Passing the endotracheal tube can be challenging in patients with significant floor of mouth or tongue edema or those with poor cardiopulmonary reserve. In such patients, it may be safer to consider tracheostomy instead.
 Figure 3. Submental Intubation. Left picture demonstrates intraoperative usage of submental intubation to allow for LeFort with medial buttress involvement and mandible fracture repairs. Right picture demonstrates the cosmetically optimal thin scar along the submental region that is well camouflaged.
Figure 3. Submental Intubation. Left picture demonstrates intraoperative usage of submental intubation to allow for LeFort with medial buttress involvement and mandible fracture repairs. Right picture demonstrates the cosmetically optimal thin scar along the submental region that is well camouflaged.
Betadine paint is applied intraorally and externally on the bilateral face and neck to prepare for any unforeseen external approaches. Usually, an intraoral vestibular approach provides adequate access to the symphysis, parasymphysis, and body fractures. Additional external transbuccal approaches using the trochar may be necessary to improve exposure for fractures located in the posterior body, angle, and subcondylar regions. External approaches are typically reserved for subcondylar fractures requiring open repair using a Risdon incision for instance, or when a reconstruction plate is being applied for comminuted or severely displaced fractures.
Prior to making incisions, lidocaine with epinephrine injections are used to promote hemostasis and hydrodissection of soft tissue away from the bone. In this particular case, local was not injected initially while assessing viability of the mucosa surrounding the open fracture site in case mucosal debridement is required to achieve reliable mucosal closure. Once we have determined that mucosa bleeds appropriately and no mucosa or soft tissue debridement is required, we then injected local to enhance hemostasis.
The first step is obtaining adequate exposure of all the fractures. A vestibular incision is made into a subperiosteal tissue plane over the left parasymphyseal region, with care to maintain around 2–3 mm of mucosal cuff for watertight closure at the conclusion of the case. The subperiosteal dissection is carried out all the way down to the inferior border of the mandible using a periosteal elevator. The inferior border of the mandible and the bony alignment along the fracture line serves as visual references for proper reduction.
For the mandibular body fracture, the vestibular incision may be extended posteriorly towards the angle. Excess mucosal overhang (wider than 2–3 mm from dentition) in this area should be avoided to optimize fracture and hardware visualization. Subperiosteal dissection is again carried down to the inferior border of the mandible and, if necessary, the posterior border of the mandible, as these borders serve as visual references for bone reduction.
In exposing either a parasymphyseal or body fracture, one must be mindful of the mental nerve, a terminal branch of the inferior alveolar nerve (cranial nerve V3). It provides sensory innervation to the ipsilateral lower face, lower lip, and mandibular teeth. The mental foramen is a weak region prone to fracture and is typically located between the first and second premolar teeth.11 The nerve can be injured during submucosal dissection. In situations with difficulty in identifying the nerve, the mental foramen should first be identified by dissecting in the subperiosteal tissue plane near midline to out laterally. Once the mental foramen is identified, the mental nerve can be followed more distally to perform safe submucosal dissection without injuring the nerve.
Once all the fractures are exposed, dental extraction and bone debridement is performed, if indicated. In cases involving bony fragments, loose pieces of bone that are not attached to the periosteum are removed down to healthy bleeding bone. If damaged dentition or alveolar fractures are encountered, consultation with an oral maxillofacial surgery team can aid in the decision to remove damaged teeth intraoperatively or consider dental rehabilitation. In this particular case, the tooth root was fractured and was assessed to be nonviable. Tooth extraction was performed to prevent delayed odontogenic infection that can lead to future hardware infection. A major downside of tooth extraction is that it leaves a gap in the bone, which can contribute to structural instability, especially with multiple adjacent fractures.
Next, MMF was performed to restore premorbid occlusion. In this case, intermaxillary fixation (IMF) screws were used to enable temporary, intraoperative fixation to maintain preoperative occlusion during open reduction. When placing IMF screws, tooth roots must be avoided by assuming that the dental root length is approximately twice the crown height with IMF screws placed in between expected tooth roots. An advantage of using a manual torque screwdriver as opposed to using a power-driven screwdriver for IMF screws is that the operator is provided with increased tactile feedback if tooth roots are inadvertently encountered during screw placement. If this occurs, the direction of screw placement can be adjusted to avoid injury.
Next, ORIF is performed starting with the fracture that is most easily reducible providing easier visualization and less comminution. Fractures within a dentate segment should always be fixated first. If multiple dentate segment fractures are present, the least comminuted or most anterior fracture should be fixated first. Anterior mandible fractures, such as parasymphyseal fractures, are generally easier to plate than body, angle, or subcondylar fractures. The reason for starting with rigid fixation of an easier fracture is that any errors in bone reduction from the first fracture repair will result in compounding bone reduction error in subsequent fracture sites and cause malocclusion.
In this case, the left parasymphyseal fracture was addressed first. Bone reduction was further refined by compressing the fractures against each other using bone reduction forceps. During this process, the inferior border of the mandible and premorbid occlusion is used to confirm proper bone reduction. In this specific case, the fracture was plated using two locking four-hole 1-mm profile miniplates utilizing two locking screws on either side of the fracture with one plate along the alveolar surface (monocortical screws) and one along the basal surface (bicortical screws). Using depth gauges, the proper length of the bicortical screws can be measured for the inferior border plate.
After proper reduction and fixation of the parasymphyseal fracture, the right body fracture was approached. In this case, to counteract the torsional forces for the body fracture, a three-dimensional locking ladder plate was used.12 Alternatively, one can place two separate miniplates. The advantage of a three-dimensional ladder plate is the additional stability between the inferior and superior plates, which are fused. This facilitates placement of two separate plates in poorly visualized areas (such as posterior body or angle fractures). A third option includes the use of a load bearing reconstruction plate at the inferior border of the body fracture, which is strong enough to resist both compressive and splaying forces, with or without an arch bar. In this case, because of the additional exposure needed for proper screw placement, a transbuccal trocar approach was used. During the trocar placement, a small skin incision is made parallel to the path of any facial nerve branches right over the center of the plate, and a blunt instrument is used to dissect intraorally. Once the hardware was secured, the patient was taken out of MMF, and restoration of premorbid occlusion was confirmed.
Lastly, watertight mucosal closure was performed. To prevent hardware infection, saliva exposure should be minimized. In cases with significant mucosal laceration or poor tissue quality, sutures can be looped around the tooth along the lingual aspect to provide a stronger anchoring suture and to avoid the incision dehiscing from buccal traction. Prior to closure, copious intraoral irrigation with Betadine paint and normal saline is performed. Deeper structures including the mentalis muscle, which is the only elevator of the lower lip and chin, should be resuspended to prevent long-term chin ptosis.9, 13 Resuspending the deeper structures also provides an additional vascularized layer to decrease the risk of hardware extrusion and wound breakdown. Mucosa is then closed with absorbable sutures, such as interrupted Vicryl in this case. To improve the watertight closure, Dermabond (cyanoacrylate adhesive) is often used by the senior author (TL) to seal the mucosal wound, acting as a suture adjunct while providing bacteriostatic and hemostatic properties.14–16
Discussion
This case represents a relatively common type of facial trauma. In this section, we will discuss key concepts that influenced the treatment plan for this particular patient. Firstly, we will discuss the biomechanics of mandible fractures that are unique to each subsite and demonstrate commonly utilized plate configurations for these fracture sites. Understanding predominant bone displacement patterns unique to each fracture site will determine the optimal hardware configuration.
A parasymphyseal fracture is any fracture that spans from canine to canine. Based on biomechanical studies, a common bony displacement pattern that occurs at the parasymphysis or symphysis is that the basal (inferior) border of the mandible widens, while the alveolar (superior) border of the mandible compresses (Figure 4A).17 As such, during ORIF, the inferior border plate is prioritized, as it provides most of the structural stability to counteract splaying forces. One can provide additional stability by using a thicker, load bearing plate or using a plate with additional screw holes.18–20
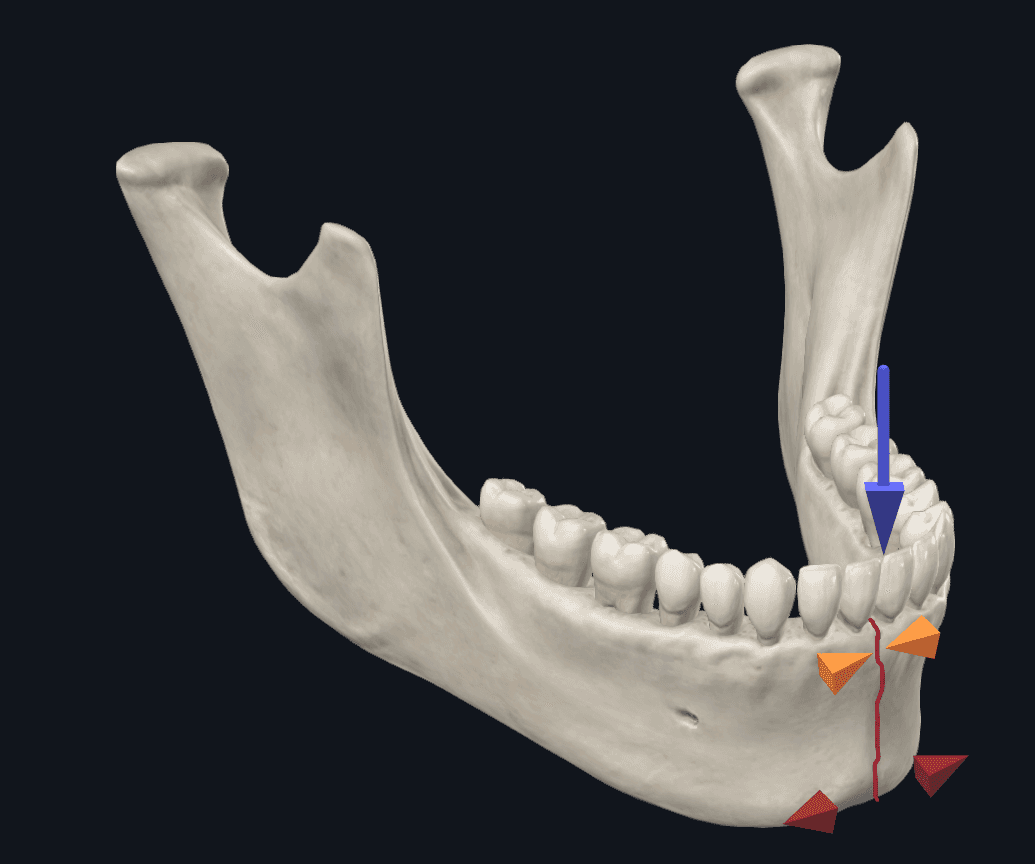
Figure 4A. Biomechanics of Symphyseal fractures. With incisor loading, there is a tendency for the inferior border of the mandible to widen while the superior border of the mandible will compress.
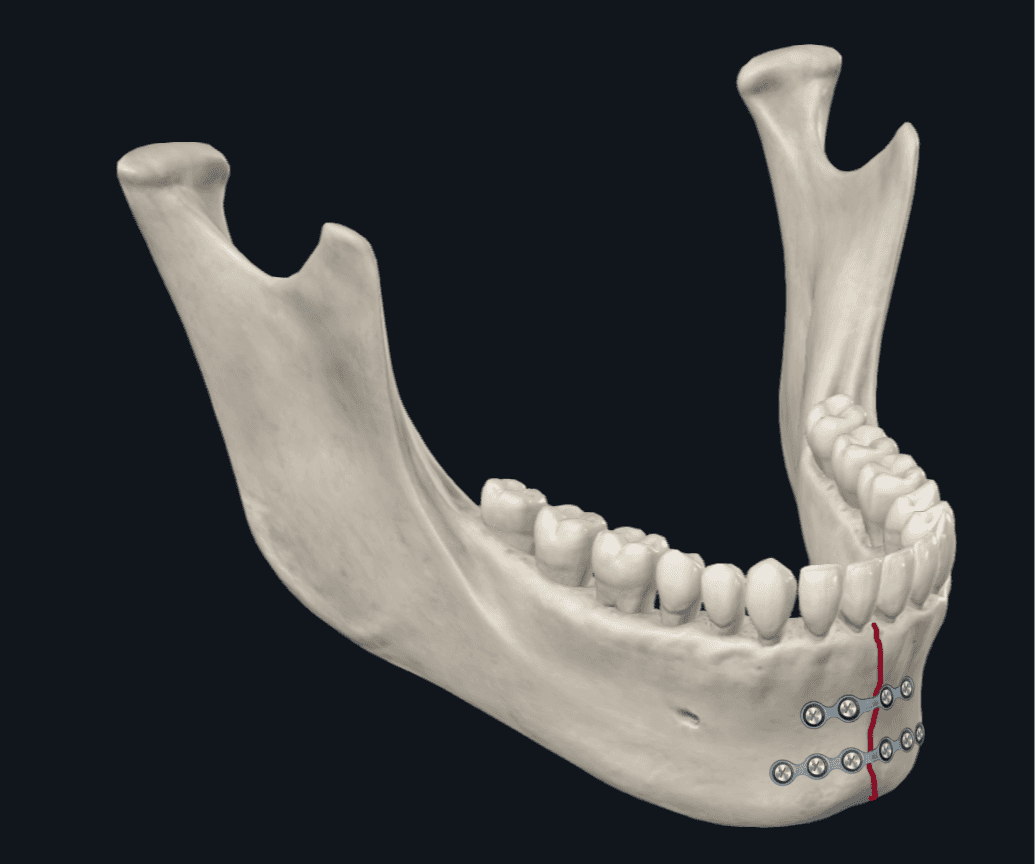
Figure 4B. Parasymphysis Plating Configuration. The emphasis is placed on plating along the inferior border plate. One can consider using two miniplates (1-mm thickness profile) with the inferior border plate being a 6-hole plate instead of 4-hole plate if additional stability is desired.
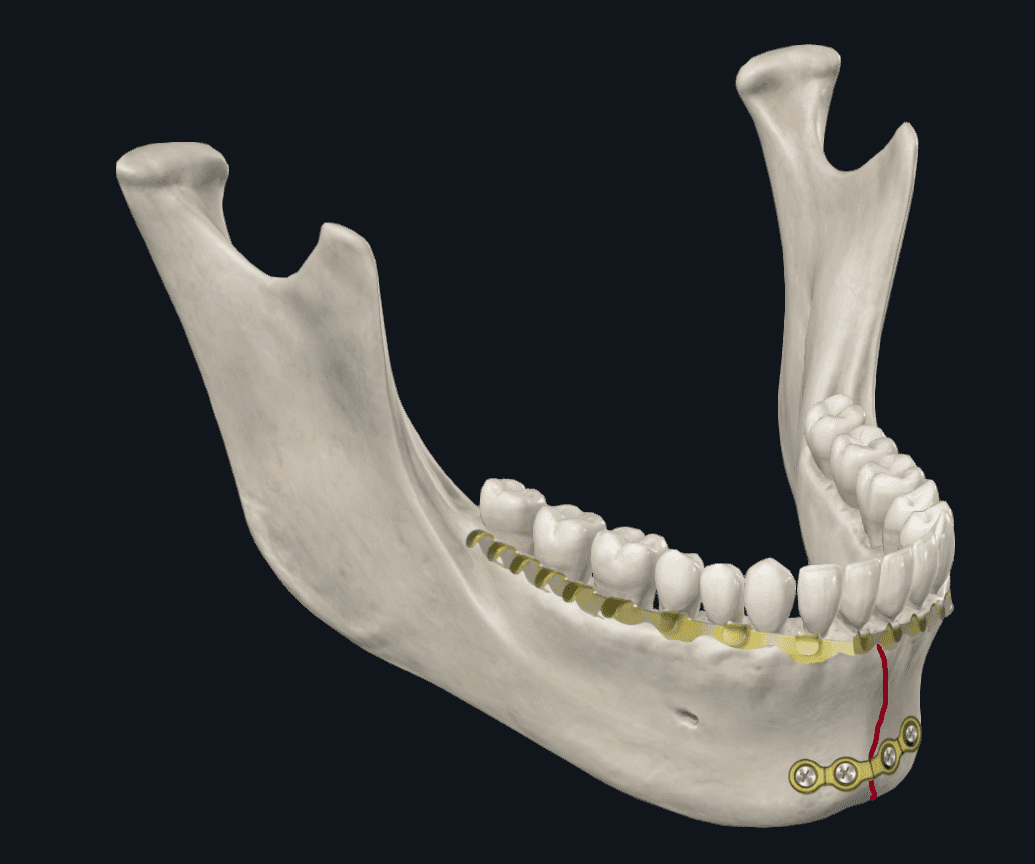
Figure 4C. Parasymphysis Plating Configuration. Alternatively, a thicker (2-mm thickness profile) single inferior border plate can be used with an arch bar that acts as a tension band, which provides added stability along the superior border of the mandible.
Contrastingly, angle fractures with incisor loading forces tend to cause widening along the alveolar border and compression at the basal border (Figure 5A). The idea behind the Champy plate is that it provides sufficient stability by plating against splaying forces along the superior border alone. However, with molar loading at the angle, there is an opposite tendency along the basal border to widen, while the alveolar border compresses (Figure 5B).17 A biomechanical study by Abraha et al. compared the use of a single alveolar border plate (Champy fixation) to biplanar fixation with a second inferior border plate during a simulation of angle fracture repairs, and found that the biplanar fixation technique provided superior stability.21, Similarly, Alkan et al. found that 3D curved angle strut plate provided more favorable biomechanical stability than the Champy plate but was not significantly different than the biplanar plate placement.12 For angle fractures, the senior author (TL), therefore, prefers the use of a three-dimensional plate with 5 or 6 holes along the superior border plate and 4 holes along the inferior border plate, placed through a transbuccal trocar approach (Figure 5C).
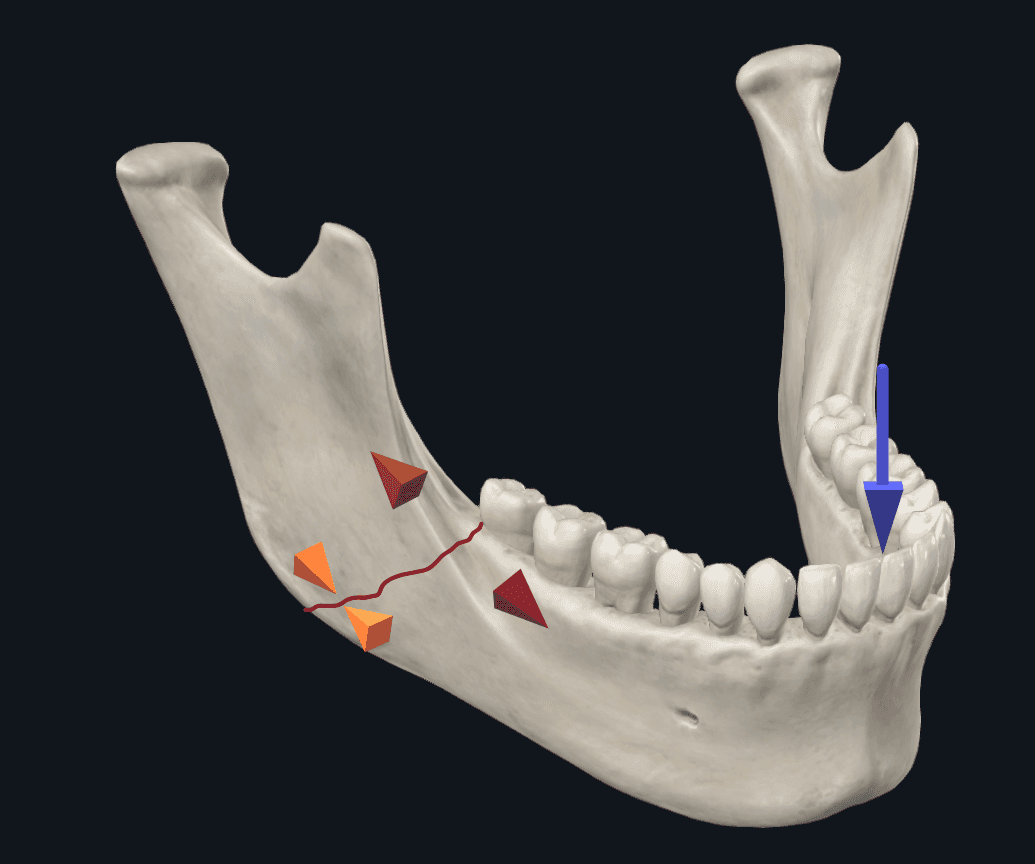
Figure 5A. Angle Fracture Biomechanics with Incisor Loading. Incisive loading results in splaying forces along the superior border and compression along the inferior border.
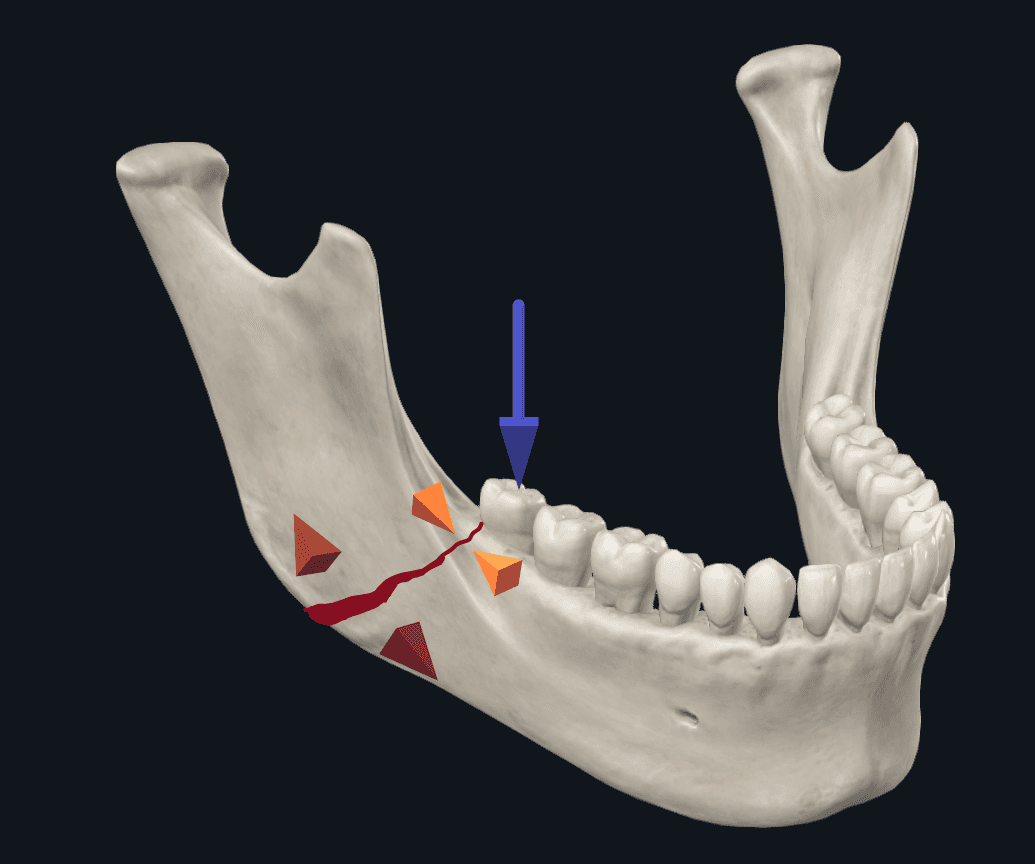
Figure 5B. Angle Fracture Biomechanics with Molar Loading. Molar loading results in compression along the superior border, while the inferior border will widen.
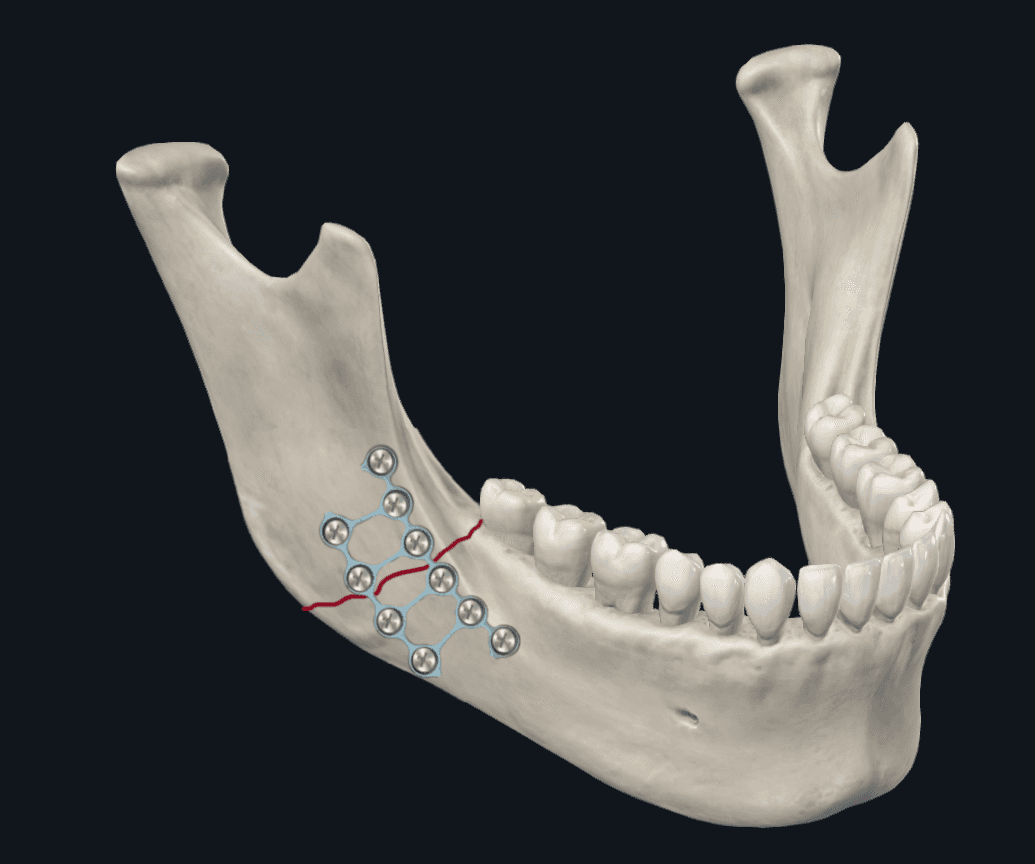
Figure 5C. Angle Plate Configuration. This shows the use of a three-dimensional ladder plate, which links the alveolar and basal plates.
The mandibular body is a transition zone between the mandibular angle and parasymphysis. As such, torsional forces predominate in this region along with either inferior or superior border displacement dictated by how anterior or posterior the loading forces are located (Figure 6A).17 Biomechanical studies looking at plate configuration recommend stabilizing a body fracture with two plates instead of a single plate to address the torsional displacement that can occur in this region.22 The senior author (TL) prefers placement of two miniplates or a three-dimensional plate for body fractures (Figure 6B). An alternative plating configuration used by the senior author (DH) is to place one thicker plate at the inferior border along with an arch bar on the mandibular dentition to compress the alveolar aspect of the fracture, resisting both compressive and splaying forces (Figure 6C). This offers the advantage of avoiding screw placement of the alveolar plate, which can potentially injure teeth roots. There is also a decreased risk of alveolar plate exposure secondary to wound dehiscence.
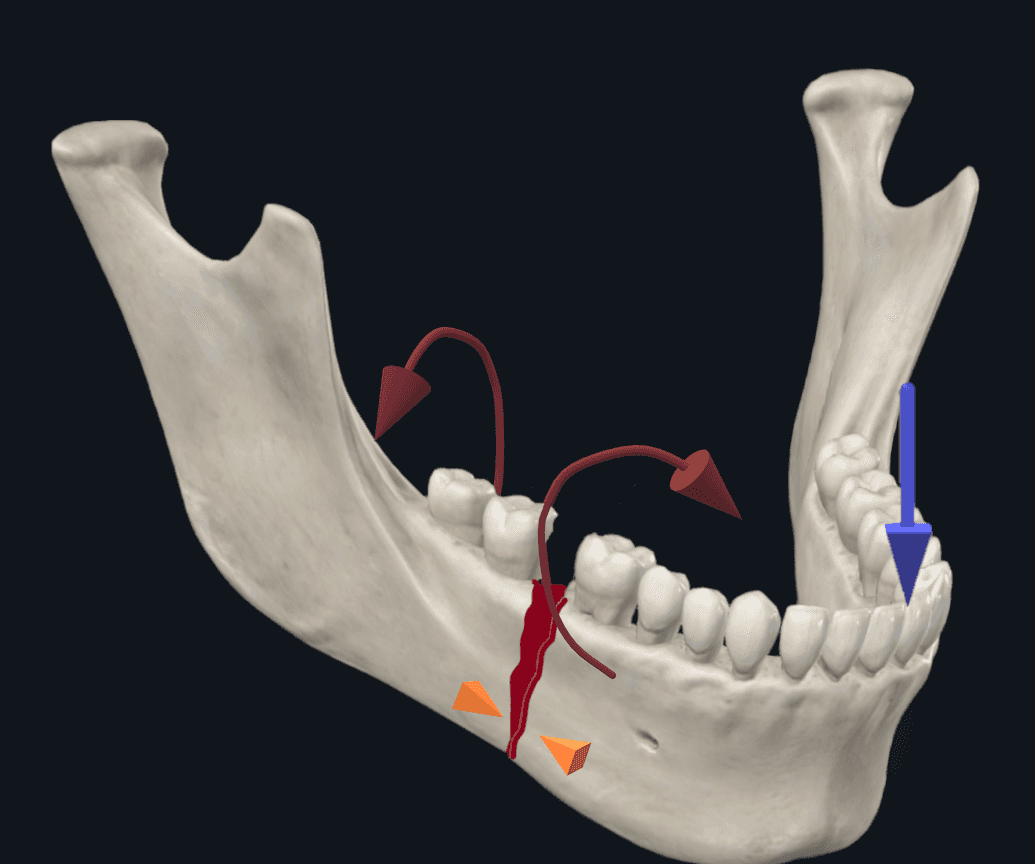
Figure 6A. Mandibular body fracture. Body fractures experience compression along the inferior/basal border with splaying at the alveolar border. These are additional opposing torsional forces on the segments anterior and posterior to the fracture line.
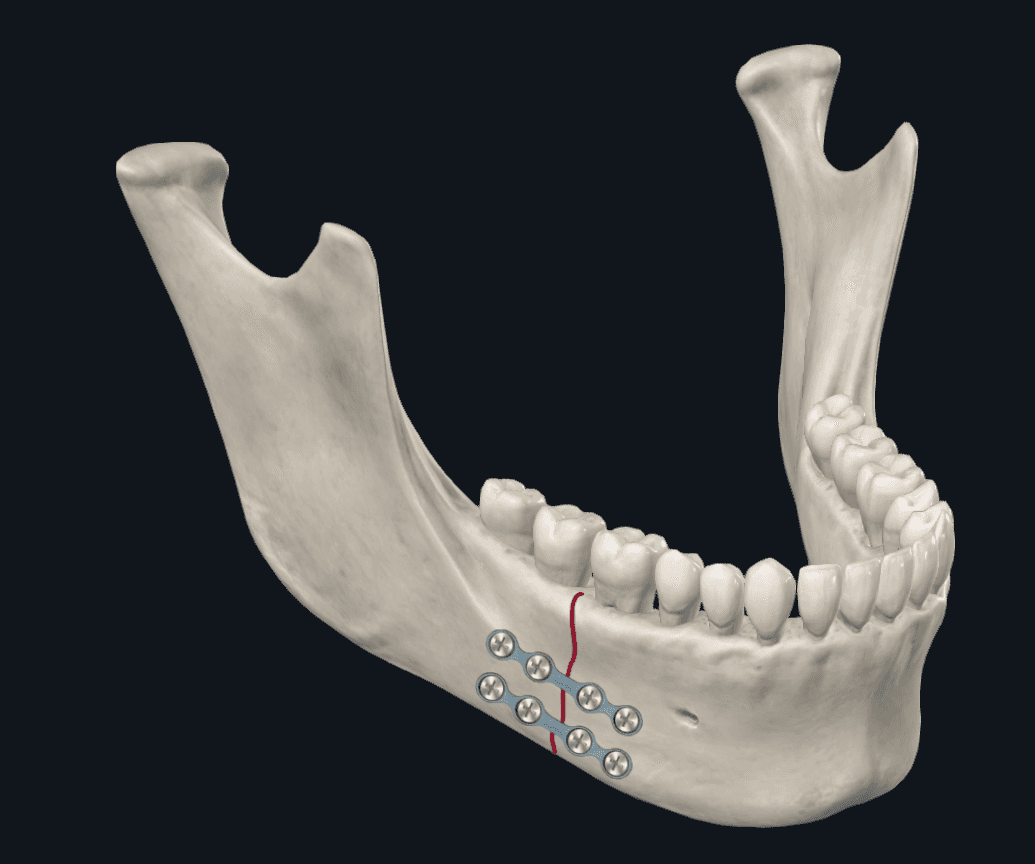
Figure 6B. Body Fracture Plating. Configuration using two miniplates.
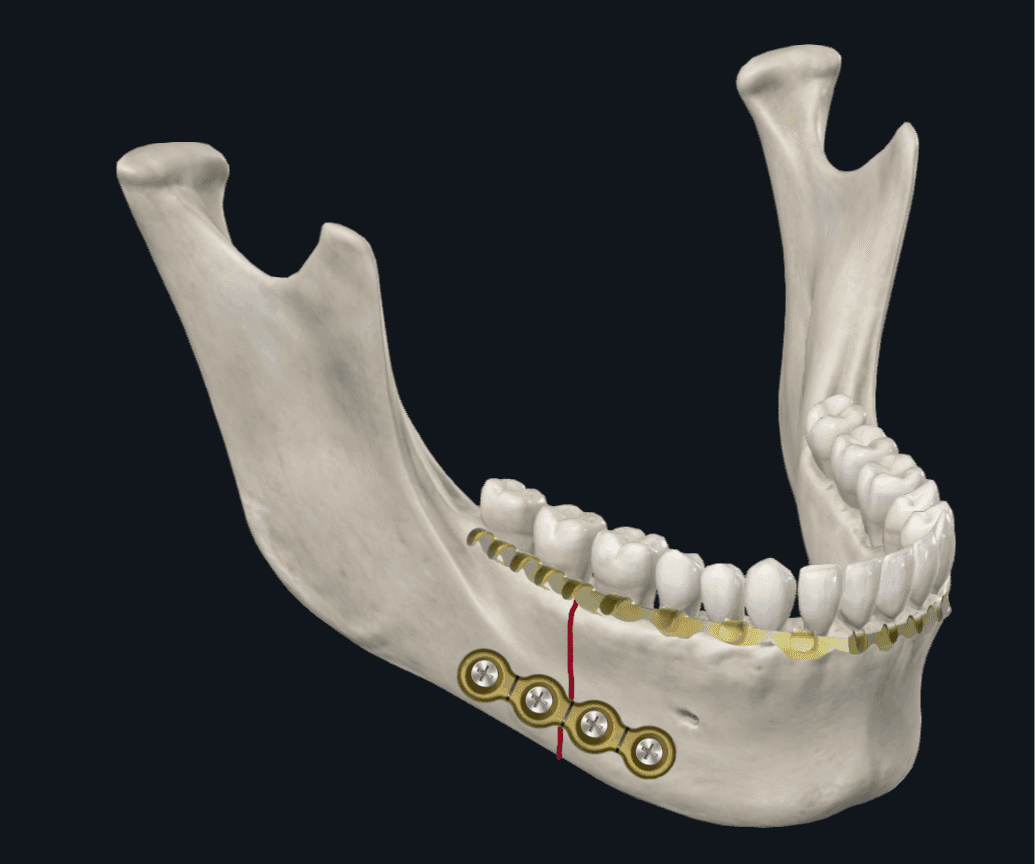
Figure 6C. Body Fracture Plating. Configuration using a single thicker inferior border plate and arch bar on the mandibular dentition.
Fixation Techniques
Once a surgeon is familiar with the biomechanics of individual fracture sites, selecting the right type of hardware is crucial for overall success of the surgery. For non-comminuted fractures with adequate bone stock present on both sides of the fracture line, miniplates have become a standard method of providing ORIF. These are considered a load-sharing type of hardware, which means the load is shared between the hardware and the bone during the bone healing process.
However, for comminuted fractures or segmental bony defects with inadequate bone stock present on either side of the fracture line, a load bearing type of plate is used, which is commonly referred to as a reconstruction plate. With the load bearing type of hardware, the entire force of loads is withstood by the hardware.
Miniplates
In the setting of craniofacial trauma, when compared to outdated compression plates, miniplates offer improved bone adaptability without needing bicortical screw fixation. This promotes semi-rigid fixation (load-sharing), leading to improved cortical bone perfusion and the formation of appropriate bony callus during healing.23
Miniplates come with either locking or non-locking versions. Locking miniplates minimize movement between the plate and bone by securing the screw head threads to a threaded plate. During tightening, this stabilizes bony segments without pulling them toward the plate and reduces the risk of bone necrosis that can occur from excessive compression on the bone surface. A major advantage is that locking plates provide adequate rigid fixation even with suboptimal plate adaptation with margins of error ranging from 0–3 mm of plate offset from the bone surface. Non-locking plates on the other hand show significant weakening (yield load, yield displacement and stiffness) even with 1 mm of plate offset.24 The screw should ideally be tightened perpendicular to the plate; however, most modern locking hardware systems tolerate up to 10–30 degrees of deviation depending on the manufacturer.6 A drawback is potentially increased hardware cost as locking screws typically cost more than nonlocking screws. However, the increase in hardware cost may be neutralized by a decrease in operative time related cost. Another disadvantage to the locking system is a loss of tactile feedback of the screw tightening into bone, which is only provided by the torque felt from the screw locking directly onto the plate.
Non-locking systems differ in mechanism by securing the plate flush against the bone. This tightening capability poses a theoretical risk of reducing blood supply to the underlying bone which can lead to bone necrosis and premature hardware failure. Precise adaptation of the plate onto the bone contact surface is mandatory to prevent improper fixation caused by minor force transfers.9, 20, 24, 25 This tends to result in longer operative times spent on achieving perfect plate adaption and may create a significant challenge in subcondylar and angle fractures where visualization and surgical access are limited. Systematic reviews comparing plates of the same dimensions, fixation principles, and design have demonstrated that in the short term, locking plates required fewer instances of postoperative MMF fixation, but yield similar overall complication rates.6, 9, 20, 2529 Although the senior author (TL) generally prefers to use a locking system for the vast majority of his cases, each case should be tailored, considering cost and ease of placement in line with the surgeon's expertise and preference.
The biomechanics of screw placement and fracture stability dictates the total number of screws that should be placed. Generally, 4-hole plates with 2 screws on either side of a fracture is adequate for non-comminuted fractures with sufficiently healthy bone stock. However, 6-hole plates with 3 screws on either side of the fracture provide significantly greater structural stability.30 A biomechanical study by Haug et al demonstrated that using three screws on either side of the fracture line provides significantly more stability than using two screws on either side. However, using 4 screws on either side of the fracture line provides marginally improved stability when compared to using 3 screws on either side.30 Therefore, 3 screws on either side of the fracture line should be utilized for less stable fractures requiring additional support.
Conventional practice dictates the use of monocortical screws at the alveolar border to prevent inadvertent injury to dental roots and the inferior alveolar nerve. It is important to remember that there is an inherent risk of injury to these structures from drilling alone.18 Tooth roots, particularly in the body region, are in close proximity to the buccal (outer) cortical bone, typically around 2–2.5 mm in depth.31 Bicortical fixation on the other hand provides theoretically improved stability to facilitate healing, however, carries potential risks of inadvertent tooth root and inferior alveolar nerve injury. Biomechanical models indicate that both monocortical and bicortical screws can achieve and maintain adequate bony reduction without significant differences in mandibular displacement from both incisor and molar loading.23 Ultimately, the decision should be based on surgeon discretion and evaluation of whether bicortical screws can be safely employed in specific instances.
Lag Screws
Another method of rigid fixation includes the use of lag screws, particularly in bony fragments that have cortical overlap or oblique orientations.6 This was popularized in 1976 for use in non-comminuted parasymphyseal fractures without significant gaps.6, 31, 32 These screws contain threads that engage only in the distal bone fragment, compressing bone between distal segment and screw head. The lag screw technique was shown to have slight superiority compared to the other fixation methods to resist force loading at the molar teeth.6, 19, 33, 34 Either 1 single lag screw with an arch bar or 2 lag screws without MMF can be a good way to secure anterior mandibular fractures.31-33 Nonetheless, placing lag screws perpendicular to fracture lines is technically challenging and relies on screw availability and surgeon expertise, making them less commonly employed.
Reconstruction Plates
Another alternative for fracture repair involves using a thicker reconstruction plate for its “load bearing” capacity.6, 35 Reconstruction plating is used in comminuted fractures and segmental bony defects. These plates remove extrinsic forces that act on the bone at tension zones, where fragment separation occurs. Biomechanical studies indicate that reconstruction plates match lag screws in resisting torsional loads, outperforming ladder plates and parallel miniplates.18, 19, 34 This thicker plate may be superior to using 2 separate miniplates for elderly or female patients with shorter mandibular vertical heights or atrophic mandibles.18 Its placement, however, can be cumbersome and costly, and in most other instances, adequate stability can be achieved through the use of 2 biplanar miniplates in non-comminuted fractures. In clinical practice, its use is mainly indicated for significant mandibular defects, comminuted fractures with poor bone stock, presence of severe osteomyelitis, or segmental mandibular defects necessitating the use of their load bearing properties.6
In summary, the ideal plate configuration for parasymphysis and body fractures should be based on the biomechanics of the fracture sites as well as patient related variables. For non-comminuted parasymphyseal fractures, using either 2 or 3 screws on either side of the fracture line with miniplates is acceptable. For parasymphyseal fractures, the inferior border plate is considered more important and some authors have recommended using a single, thicker inferior plate as opposed to 2 miniplates.18 Other valid repair options include the use of lag screws. For body fractures, the key is to resist torsional forces. Using either a single three-dimensional plate versus 2 separate miniplates along the inferior and superior mandibular borders have been demonstrated to provide similar outcomes and stability. Alternatively, an arch bar can substitute for the superior plate in parasymphyseal, body, or angle fractures to minimize superior plate related complications. Finally, a single, thicker inferior plate is a traditional and time-tested approach, especially if postoperative MMF fixation is performed concurrently.18
Intraoperative Management of Teeth Within Mandible Fracture
The management of teeth along a fracture line can be challenging. Any involved teeth that are not extracted have the potential to undergo necrosis, particularly in the presence of chronic infections, which can lead to nonunion. Conversely, extracting any teeth can lead to structural instability within the remaining mandible. The senior authors advocate for a more conservative approach, emphasizing the salvage potential of viable teeth through endodontic treatments and prophylactic antibiotics. Vertical root fractures and horizontal fractures near the crown are less favorable for future endodontic care, and extraction should be considered.
In our case, the patient's tooth root was split in half, minimizing the chance of future restoration. Following consultation with an oral-maxillofacial surgeon, the tooth root was extracted. Indications for tooth removal include severe periodontal disease, unrestorable crowns, vertical root fractures, or any misaligned teeth that interfere with proper mandibular reduction.2, 9, 37
Postoperative MMF
In this particular case, only temporary MMF intraoperatively was utilized for bone reduction, in line with conventional surgical management. The use of postoperative MMF has also been a standard treatment protocol and its efficacy in promoting bone union is uncontested. However, routine postoperative MMF comes with inherent risks including airway compromise, gingival injury, temporomandibular joint immobility or ankylosis, difficulty with oral hygiene, and patient non-compliance or dissatisfaction. A study by Saman et al. analyzed 413 mandible fractures (non-comminuted symphyseal, parasymphyseal, or angle fractures). Among the patients, 54% were treated with postoperative MMF, while the remaining 46% were not. The study found no significant differences in wound dehiscence, infection, plate removal, nonunion, malunion, and malocclusion, supporting selective usage of postoperative MMF in line with current retrospective studies.
Postoperative MMF may be beneficial for severely comminuted or segmental mandibular defects. Rigid MMF followed by elastics can also maintain proper occlusion during healing for minimally-displaced subcondylar fractures or condylar head fractures not amenable to screw placement. Patients with true condylar head or intracapsular fractures should ideally be placed in MMF for the shortest time frame allowable to achieve premorbid occlusion.39 Similarly, patients who have residual minor occlusal discrepancies may also benefit from a short period (1–2 weeks) of MMF to allow for healing.38, 40, 41 MMF is not recommended for patients who are non-compliant, psychiatrically or neurologically obtunded, or have seizure or nausea and vomiting disorders, severe airway or pulmonary disease, or intellectual disability.42
Equipment
Stryker craniofacial mandible plating set.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Motamedi MH. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J Oral Maxillofac Surg. Jan 2003;61(1):61-4. doi:10.1053/joms.2003.50049.
- Rahpeyma A, Khajehahmadi S, Abdollahpour S. Mandibular symphyseal/parasymphyseal fracture with incisor tooth loss: preventing lower arch constriction. Craniomaxillofac Trauma Reconstr. Mar 2016;9(1):15-9. doi:10.1055/s-0035-1551542.
- King RE, Scianna JM, Petruzzelli GJ. Mandible fracture patterns: a suburban trauma center experience. Am J Otolaryngol. Sep-Oct 2004;25(5):301-7. doi:10.1016/j.amjoto.2004.03.001.
- Koshy JC, Feldman EM, Chike-Obi CJ, Bullocks JM. Pearls of mandibular trauma management. Semin Plast Surg. Nov 2010;24(4):357-74. doi:10.1055/s-0030-1269765.
- Jain P, Rathee M. Mandible Body Fracture. [Updated 2023 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553119/.
- A. Y. Principles of Internal Fixation in Maxillofacial Surgery. In: Bonanthaya K, Panneerselvam E, Manuel S, Kumar VV, Rai A, eds. Oral and Maxillofacial Surgery for the Clinician. Springer Nature; 2021.
- Barker DA, Park SS. Is fixation of mandible fractures urgent? Laryngoscope. May 2011;121(5):906-7. doi:10.1002/lary.21777.
- James J, Farrell Tt, Stevens M, Looney S, Faigen A, Anderson J. Time to open repair of mandibular fractures and associated complications. J Oral Maxillofac Surg. Jan 2020;78(1):101-107. doi:10.1016/j.joms.2019.09.009.
- Perez D, Ellis E III. Complications of mandibular fracture repair and secondary reconstruction. Semin Plast Surg. Nov 2020;34(4):225-231. doi:10.1055/s-0040-1721758.
- Webb LS, Makhijani S, Khanna M, et al. A comparison of outcomes between immediate and delayed repair of mandibular fractures. Can J Plast Surg. Winter 2009;17(4):124-6. doi:10.1177/229255030901700401.
- Loyal PK, Butt F, Ogeng'o JA. Branching pattern of the extraosseous mental nerve in a kenyan population. Craniomaxillofac Trauma Reconstr. Dec 2013;6(4):251-6. doi:10.1055/s-0033-1356756.
- Alkan A, Celebi N, Ozden B, et al. Biomechanical comparison of different plating techniques in repair of mandibular angle fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(6):752-6.
- Shah A, Patel A, Steinbacher D. Soft tissue coverage for mandibular fractures using two miniplates. Craniomaxillofac Trauma Reconstr. Dec 2012;5(4):253-4. doi:10.1055/s-0032-1329543.
- Borie E, Rosas E, Kuramochi G, Etcheberry S, Olate S, Weber B. Oral applications of cyanoacrylate adhesives: a literature review. Biomed Res Int. 2019;2019:8217602. doi:10.1155/2019/8217602.
- Kazzi MG, Silverberg M. Pediatric tongue laceration repair using 2-octyl cyanoacrylate (dermabond((R))). J Emerg Med. Dec 2013;45(6):846-8. doi:10.1016/j.jemermed.2013.05.004.
- Sagar P, Prasad K, Lalitha RM, Ranganath K. Cyanoacrylate for intraoral wound closure: a possibility? Int J Biomater. 2015;2015:165428. doi:10.1155/2015/165428.
- Tams J, van Loon JP, Otten E, Rozema FR, Bos RR. A three-dimensional study of bending and torsion moments for different fracture sites in the mandible: an in vitro study. Int J Oral Maxillofac Surg. Oct 1997;26(5):383-8. doi:10.1016/s0901-5027(97)80803-x.
- Ellis E, 3rd. A study of 2 bone plating methods for fractures of the mandibular symphysis/body. J Oral Maxillofac Surg. Jul 2011;69(7):1978-87. doi:10.1016/j.joms.2011.01.032.
- Madsen MJ, McDaniel CA, Haug RH. A biomechanical evaluation of plating techniques used for reconstructing mandibular symphysis/parasymphysis fractures. J Oral Maxillofac Surg. Oct 2008;66(10):2012-9. doi:10.1016/j.joms.2008.06.013.
- Lee T, Sawhney R, Ducic Y. Miniplate fixation of fractures of the symphyseal and parasymphyseal regions of the mandible: a review of 218 patients. JAMA Facial Plast Surg. Mar 1 2013;15(2):121-5. doi:10.1001/jamafacial.2013.307.
- Mehari Abraha H, Iriarte-Diaz J, Reid RR, Ross CF, Panagiotopoulou O. Fracture fixation technique and chewing side impact jaw mechanics in mandible fracture repair. JBMR Plus. Jan 2022;6(1):e10559. doi:10.1002/jbm4.10559.
- De Medeiros RC, de Moura AL, Sawazaki R, et al. Comparative in vitro mechanical evaluation of technique using a 2.0 mm locking fixation system for simulated fractures of the mandibular body. J Craniomaxillofac Surg. 2015 Apr;43(3):302-5. doi:10.1016/j.jcms.2014.11.012.
- Joshi U, Kurakar M. Assessment of lingual stability in mandible fracture: monocortical versus bicortical fixation using FEM analysis. J Maxillofac Oral Surg. Dec 2018;17(4):514-519. doi:10.1007/s12663-017-1073-0.
- Haug RH, Street CC, Goltz M. Does plate adaptation affect stability? A biomechanical comparison of locking and nonlocking plates. J Oral Maxillofac Surg. Nov 2002;60(11):1319-26. doi:10.1053/joms.2002.35732.
- Harjani B, Singh RK, Pal US, Singh G. Locking v/s non-locking reconstruction plates in mandibular reconstruction. Natl J Maxillofac Surg. Jul 2012;3(2):159-65. doi:10.4103/0975-5950.111371.
- Batbayar EO, Dijkstra PU, Bos RRM, van Minnen B. Complications of locking and non-locking plate systems in mandibular fractures. Int J Oral Maxillofac Surg. Sep 2019;48(9):1213-1226. doi:10.1016/j.ijom.2019.02.019.
- Collins CP, Pirinjian-Leonard G, Tolas A, Alcalde R. A prospective randomized clinical trial comparing 2.0-mm locking plates to 2.0-mm standard plates in treatment of mandible fractures. J Oral Maxillofac Surg. Nov 2004;62(11):1392-5. doi:10.1016/j.joms.2004.04.020.
- Herford AS, Ellis E III. Use of a locking reconstruction bone plate/screw system for mandibular surgery. J Oral Maxillofac Surg. Nov 1998;56(11):1261-5. doi:10.1016/s0278-2391(98)90605-x.
- Sarkar DF, Mishra N, Samal D, et al. Locking versus non-locking plating system in the treatment of mandibular fractures: a randomized comparative study. J Craniomaxillofac Surg. Mar 2021;49(3):184-190. doi:10.1016/j.jcms.2021.01.006.
- Haug RH. The effects of screw number and length on two methods of tension band plating. J Oral Maxillofac Surg. Feb 1993;51(2):159-62. doi:10.1016/s0278-2391(10)80015-1.
- Al-Jandan BA, Al-Sulaiman AA, Marei HF, Syed FA, Almana M. Thickness of buccal bone in the mandible and its clinical significance in mono-cortical screws placement. A CBCT analysis. Int J Oral Maxillofac Surg. Jan 2013;42(1):77-81. doi:10.1016/j.ijom.2012.06.009.
- Niederdellmann H, Schilli W, Duker J, Akuamoa-Boateng E. Osteosynthesis of mandibular fractures using lag screws. Int J Oral Surg. Jun 1976;5(3):117-21. doi:10.1016/s0300-9785(76)80059-2.
- Ellis E III, Ghali GE. Lag screw fixation of anterior mandibular fractures. J Oral Maxillofac Surg. Jan 1991;49(1):13-21; discussion 21-2. doi:10.1016/0278-2391(91)90259-o.
- Emam HA, Stevens MR. Can an arch bar replace a second lag screw in management of anterior mandibular fractures? J Oral Maxillofac Surg. Feb 2012;70(2):378-83. doi:10.1016/j.joms.2011.08.010.
- Richardson M, Hayes J, Jordan JR, Puckett A, Fort M. Biomechanical evaluation of a mandibular spanning plate technique compared to standard plating techniques to treat mandibular symphyseal fractures. Surg Res Pract. 2015;2015:569030. doi:10.1155/2015/569030.
- Coletti DP, Caccamese JF Jr, Norby C, Edwards S, von Fraunhofer JA. Comparative analysis of the threaded and tapered locking reconstruction plates. J Oral Maxillofac Surg. Dec 2007;65(12):2587-93. doi:10.1016/j.joms.2006.05.054.
- Kumar PP, Sridhar BS, Palle R, Singh N, Singamaneni VK, Rajesh P. Prognosis of teeth in the line of mandibular fractures. J Pharm Bioallied Sci. Jul 2014;6(Suppl 1):S97-S100. doi:10.4103/0975-7406.137397.
- Spinnato G, Alberto PL. Teeth in the line of mandibular fractures. Atlas Oral Maxillofac Surg Clin North Am. Mar 2009;17(1):15-8. doi:10.1016/j.cxom.2008.10.006.
- Saman M, Kadakia S, Ducic Y. Postoperative maxillomandibular fixation after open reduction of mandible fractures. JAMA Facial Plast Surg. Nov-Dec 2014;16(6):410-3. doi:10.1001/jamafacial.2014.543.
- Kumar I, Singh V, Bhagol A, Goel M, Gandhi S. Supplemental maxillomandibular fixation with miniplate osteosynthesis-required or not? Oral Maxillofac Surg. Mar 2011;15(1):27-30. doi:10.1007/s10006-010-0229-6.
- Park JM, Jang YW, Kim SG, et al. Comparative study of the prognosis of an extracorporeal reduction and a closed treatment in mandibular condyle head and/or neck fractures. J Oral Maxillofac Surg. Dec 2010;68(12):2986-93. doi:10.1016/j.joms.2010.02.034.
- Chritah A, Lazow SK, Berger JR. Transoral 2.0-mm locking miniplate fixation of mandibular fractures plus 1 week of maxillomandibular fixation: a prospective study. J Oral Maxillofac Surg. Dec 2005;63(12):1737-41. doi:10.1016/j.joms.2005.08.022.
- Ezhilarasi SKR. IMF After ORIF in maxillofacial fractures—case report and literature review. The Traumaxilla. 2022;4:1-3. doi:10.1177/26323273211073785.
- Cornelius CP, Ehrenfeld M. The use of MMF screws: surgical technique, indications, contraindications, and common problems in review of the literature. Craniomaxillofac Trauma Reconstr. Jun 2010;3(2):55-80. doi:10.1055/s-0030-1254376.






| Publication Date | 5/9/2024 |
| Article ID | 414 |
| Production ID | 0414 |
| Volume | 2024 |
| Issue | 414 |
| DOI | |
| https://doi.org/10.24296/jomi/414 | |