Carbon Fiber Implant for Fixation of a Pathologic Subtrochanteric Fracture
Abstract
Herein, we present a patient with a pathologic subtrochanteric femur fracture secondary to an undiagnosed primary lung adenocarcinoma. The fracture, occurring in the context of persistent atraumatic thigh and knee pain, prompted swift identification of its pathological nature in the Emergency Department. The treatment plan involved open reduction and internal fixation utilizing a carbon fiber nail, considering the immediate need for stabilization and underlying oncologic factors.
The primary focus was on achieving fracture fixation, traditionally accomplished with intramedullary devices. However, the decision to employ a carbon fiber nail was made due to the pathological nature of the fracture and the subsequent need for post surgery oncologic intervention. The unique radiolucency of carbon fiber aids in postoperative radiation planning, ensuring optimal visualization and precision in targeting bone lesions. This approach contributes to fracture reduction while minimizing interference with radiation therapy.
The surgical procedure involved intramedullary rodding with a carbon fiber nail, achieving successful fracture reduction and optimal hardware positioning. Histopathological assessment confirmed metastatic lung adenocarcinoma. Postoperatively, the patient received palliative radiation and targeted therapy, demonstrating substantial improvement at the two-month follow-up (Figure 6).
The case highlights the strategic use of carbon fiber implants in managing pathologic fractures, offering advantages in postoperative imaging, disease monitoring, and precision in radiation therapy planning. The multidisciplinary approach underscores the importance of considering implant selection nuances, especially in metastatic bone disease, to optimize outcomes.
Keywords
Carbon fiber implants; pathologic fracture; metastatic bone disease.
Case Overview
Background
A patient presented with a pathologic subtrochanteric femur fracture on the right side, occurring in the context of an initially undiagnosed primary lung adenocarcinoma. Her medical history included persistent atraumatic thigh and knee pain, progressively worsening, culminating in a sudden increase in pain, leg weakness, and a subsequent fall after her leg gave way on the stairs. Upon presentation to the Emergency Department, the pathological nature of the fracture was promptly identified. Subsequent to an oncologic assessment, the treatment plan involved an open reduction and internal fixation, opting for a carbon fiber nail due to the immediate need for fracture stabilization and the underlying oncologic considerations.
In this case, the primary focus was on achieving fracture fixation, a task traditionally accomplished with an intramedullary device. However, considering the pathological nature of the fracture and the subsequent need for oncologic intervention post surgery, the decision was made to utilize a carbon fiber nail. Pathologic fractures, common in metastatic conditions, often necessitate postoperative radiation to address residual cancer cells and facilitate native bone healing. The implementation of radiation treatment planning, involving CT simulation planning, is significantly aided by carbon fiber implants, enhancing visualization and precision in targeting the bone lesion. This approach aims to attain the goal of fracture reduction while minimizing the interference posed by traditional metal implants during radiation planning.
Focused History of the Patient
A geriatric white female was found to have a subtrochanteric pathologic fracture. Incidentally, on further work-up, the patient was found to have a primary lung carcinoma. Employing a carbon fiber nail during open reduction and internal fixation not only stabilized the fracture but also optimized precision in postoperative radiation planning.
Physical Exam
The patient denied any head strike or loss of consciousness and exhibited no signs of delirium or confusion. Physical examination of the right lower extremity was limited due to pain. Her right leg was noticeably shortened. The examination revealed pain and limited strength in the extensor hallucis longus (EHL), flexor hallucis longus (FHL), tibialis anterior (TA), and gastrocnemius (GS). Distal pulses, including dorsalis pedis (DP) and posterior tibial (PT), were intact, and the right foot displayed warmth and adequate perfusion. Subsequent soft tissue injury evaluation disclosed disruptions in the superficial peroneal nerve (SPN), deep peroneal nerve (DPN), tibial nerve (TN), saphenous nerve, and sural nerve.
Imaging
X-ray imaging of the right hip and femur at her initial presentation following the fall revealed a displaced subtrochanteric fracture with medial displacement of the distal fragment. The femoral head remained well-seated in the acetabulum, and the remainder of the femur was intact (Figure 1). Degenerative joint space narrowing with marginal osteophytes was evident. A contrast-enhanced computed tomography (CT) scan of the chest depicted a large right upper lobe mass encasing the right mainstem bronchus, resulting in complete right upper lobe atelectasis (Figure 2). The mass was suspicious for malignancy. Multiple enlarged mediastinal and bilateral hilar lymph nodes are concerning for metastatic disease. A non-enhanced CT scan of the right femur revealed non-specific intracortical lucencies of the femoral midshaft at the inferior margin of the fracture. This finding raised concerns for underlying permeative lesions and a pathological fracture (Figure 3). Although follow-up magnetic resonance imaging (MRI) may have helped determine the presence of underlying osseous lesions, evaluation in the acute setting is limited by edema and hemorrhage, prompting the decision to forgo this examination.
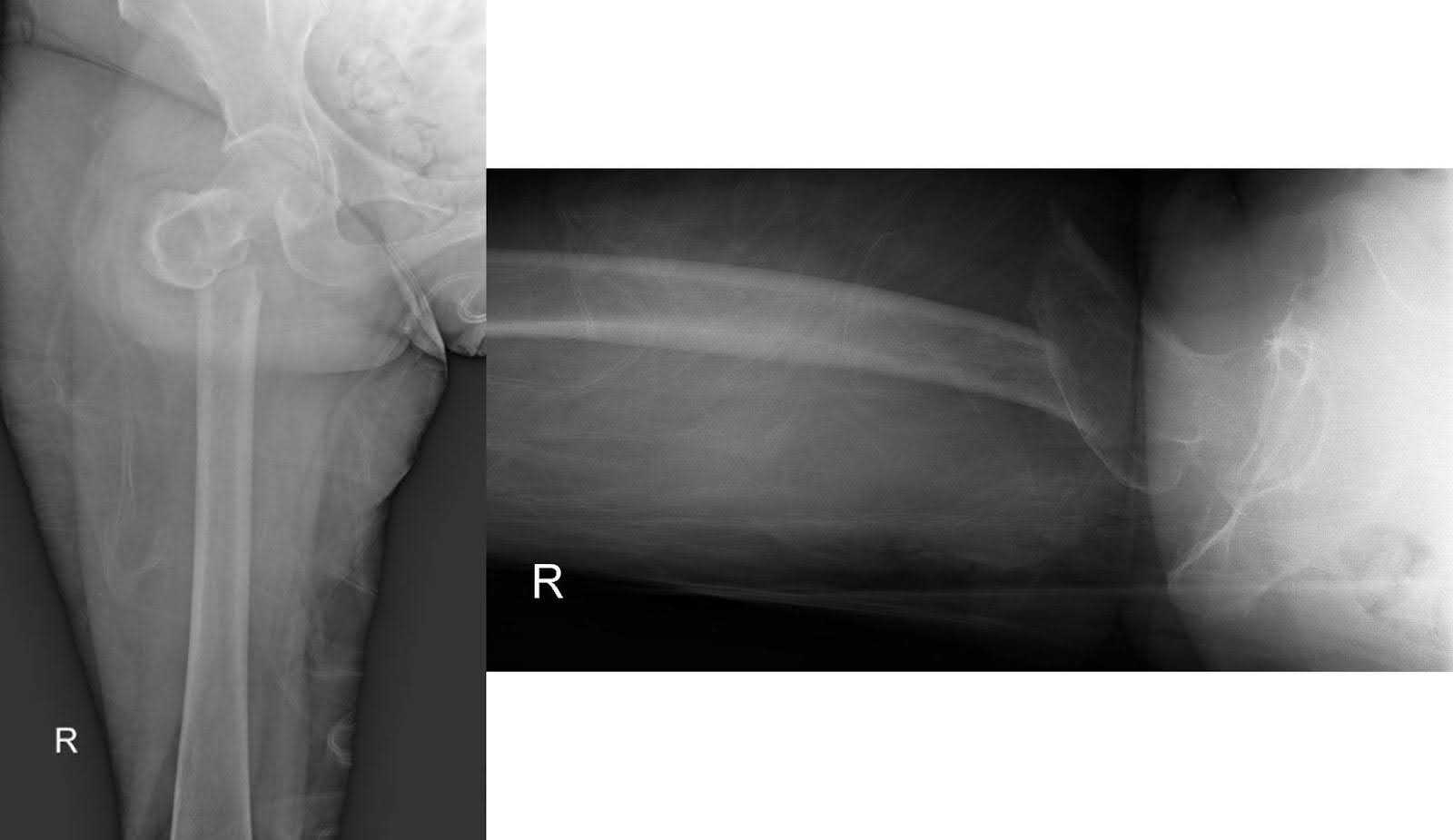
Figure 1. AP and lateral x-rays of the right hip illustrating a displaced subtrochanteric fracture. The femoral head maintains reduction within the acetabulum, while the rest of the femur remains structurally intact.

Figure 2. A heterogeneously enhancing mass, located in the right paramediastinal region of the right upper lobe, was found during a CT chest with contrast. The presence of this finding suggests a diagnosis of primary lung cancer.
 Figure 3. Lateral and AP non-contrasted CT images of the right femur show intracortical lucencies in the femoral mid-shaft, suggesting a potential pathological fracture.
Figure 3. Lateral and AP non-contrasted CT images of the right femur show intracortical lucencies in the femoral mid-shaft, suggesting a potential pathological fracture.
Natural History
Pathologic fractures, distinct from traumatic fractures, emerge as a result of an underlying condition, including but not limited to osteoporosis, cancer, infection, or metabolic disorders. This distinctive category of fractures is characterized by the influence of pathological processes that compromise the structural integrity of the bone.1 Pathological fractures can lead to significant morbidity and a decline in overall quality of life.2 The skeletal system ranks as the third most common site for metastases, following the lung and liver.3 Around 70% of all bone metastases occur due to metastatic breast and prostate cancers, with lung, kidney, and thyroid tumors being the next most common causes in terms of prevalence.4
Patients experiencing pathologic fractures may exhibit pain and swelling at the fracture site, along with difficulty ambulating, reduced range of motion, ecchymosis, local edema, and noticeable extremity shortening.5 A clinical indicator of pathologic fractures lies in their underlying cause, often presenting with minimal trauma—considerably less force than required to fracture a healthy bone.6 Although infrequent, pathologic fractures may be the presenting sign of an underlying malignancy.7 This underscores the need for meticulous investigation and diagnostic scrutiny, especially in cases where there is a history of limited or absent trauma.
A femoral pathologic fracture presents similar challenges to a traumatic femur fracture yet introduces additional postoperative considerations that impact implant selection. Similar to managing femur fractures in healthy bone, it is crucial to achieve fracture reduction and stabilization. This not only alleviates pain and provides stability for ambulation but also establishes a biomechanical environment conducive to optimal fracture healing.
Managing subtrochanteric fractures presents challenges in achieving reduction and fixation, with the reduction often requiring percutaneous or open techniques.8 Surgical fixation, a well-tolerated intervention, demonstrates comparable functional outcomes to non-pathologic fixation.9 From an oncologic perspective, treating the malignant cells in the bone is pivotal for effective bone healing. In the post fracture treatment regimen, chemotherapy and radiation therapy play crucial roles in achieving this goal. Radiation therapy, typically planned with external beam therapy, necessitates a pretreatment CT scan for accurate planning. However, the presence of metal implants can cause beam scatter, reducing imaging resolution and impacting radiation therapy plans. Carbon fiber implants, devoid of the radiographic properties of metals, can effectively fulfill the goals of fracture reduction and healing while minimally affecting adjuvant therapies essential for radiotherapy.10
Options for Treatment
The purpose of long bone fixation after a fracture is to facilitate proper healing, restore stability, and promote functional recovery. When considering treatment options for subtrochanteric femur fractures, the primary modalities of fixation include nail or plate fixation, with the current orthopedic literature favoring nail fixation.8 In the selection of implant materials, it is imperative to account for the underlying etiology of the fracture and surgeon proficiency with both techniques.
For patients with pathological fractures secondary to metastatic bone disease, carbon fiber nails may be a preferable alternative to titanium nails, owing to their radiolucency and favorable mechanical properties.11,12 Carbon fiber implants significantly decrease scatter on CT and reduce susceptibility artifact on MRI, which allows for improved visualization of bone healing, postoperative surveillance for local disease recurrence or progression, and precision in radiation planning.10,13,14
While there are several advantages to carbon fiber fixation, there are no differences in the functional outcomes and complication profiles of carbon fiber and metal fixation.11,12 Both techniques achieve the goal of fracture stabilization and maintenance of reduction with a low risk of complication and well-documented healing and biocompatibility. Consequently, the operating surgeon should carefully weigh their proficiency and comfort level with each fixation method and implant type in the decision-making process.12,15
Rationale for Treatment
When formulating the treatment strategy for a pathologic subtrochanteric fracture, it is imperative to take into account both short- and long-term goals. In the short term, utilizing a carbon fiber implant for fixation aims to establish bony stability following fracture reduction. Fracture reduction restores limb length, muscular tension, and normal anatomical relationships. Maintaining this reduction decreases pain by stabilizing bony fragments appropriately.16 As a load-sharing device, the implant may allow the patient to mobilize immediately, reducing the risk of venous thromboembolism, bed sores, and rapid deconditioning.17
In the intermediate postoperative period, the stability afforded by the implant plays a crucial role in promoting fracture healing, especially when combined with adjuvant therapy for cancer treatment.18 Opting for a carbon fiber implant not only simplifies postoperative radiographic disease monitoring but also enhances the precision of planning for radiation therapy. This strategic choice contributes to improved accuracy and efficacy in the overall treatment approach.19
Special Considerations
Carbon fiber implants may be contraindicated for humeral diaphyseal bone tumors requiring large segmental resection with a short residual bone segment (5 cm) and a substantial cement spacer. Such implants may fail via tension due to bending forces at the distal portion of the intramedullary nail, where there is a modulus of elasticity mismatch between the cement spacer and the residual bone. In such scenarios, titanium intramedullary nails emerge as a preferable choice, offering a potential solution to address the challenges associated with carbon fiber implants in this specific context.20
Surgeons need to take into account their familiarity and comfort level with carbon fiber implants, considering the learning curve associated with these implants. Carbon fiber implants have been linked to longer operative and fluoroscopy times, as well as increased blood loss, particularly in orthopedic and spine oncology.12,21 Balancing clinical considerations and surgeon proficiency is essential when deciding on the suitability of carbon fiber implants in this specialized field.
The utilization of carbon fiber implants in orthopedics demands a thorough consideration of several pivotal clinical factors. Despite comparable complication and failure rates to titanium implants, carbon fiber implants lack intraoperative flexibility for bending or contouring. Surgeons must engage in meticulous preoperative planning to ensure an optimal fit.22 While the radiolucency of carbon fiber is advantageous for postoperative imaging studies, confirming the implant position intraoperatively may pose challenges. On the contrary, metallic implants, though devoid of intraoperative flexibility, often disrupt radiation planning mapping and hinder accurate dose calculation and delivery.23,24 Furthermore, in situations where the disease extends to the joint and necessitates joint replacement, carbon fiber implants may not be the most suitable option. Therefore, the decision to employ carbon fiber implants involves a nuanced assessment of their benefits and limitations within specific clinical contexts.
Surgical Procedure
Intramedullary rodding of the right femur was performed for operative fixation of the lesion in addition to an open biopsy to determine the etiology of the metastatic bone disease. Per imaging studies, this appeared to be a primary lung cancer with metastasis to the bone. The patient was placed in a lateral decubitus with the assistance of a beanbag. All bony prominences were adequately padded. Placement of a subaxillary roll and offloading of the left peroneal nerve took place.
A lateral incision was made on the proximal thigh, and a subvastus approach was performed subsequently to expose the fracture site. A Cobra retractor facilitated exposure after identification of the fracture site. Permanent and frozen pathology samples were obtained using curettes. Frozen pathology confirmed metastatic lung adenocarcinoma. Aggressive debridement of the tumor lesion, both inside and outside the bone, was performed. Copious irrigation of the surgical field with peroxide solution was performed.
Utilizing fresh gloves and a new set of instruments, a subsequent incision proximal to the initial site was made to gain access to the proximal femur. The fascia of the gluteus medius was longitudinally incised to identify the tip of the greater tuberosity. A 3.2-mm guidewire marked the starting point, ensuring an excellent position in both anteroposterior (AP) and lateral views. Maintaining the femur in a neutral position was facilitated by a Shantz pin, aiding in internal rotation and adduction of the proximal femoral fragment.
The significantly flexed fragment underwent additional positioning to ensure extension. A finger reduction tool, supported by two Shantz pins in the proximal femur and the femoral shaft, was used to achieve anatomical reduction of the fracture. With the fracture reduced, the opening reamer was used to open the trajectory in the proximal femur. Advancing a ball-tipped guidewire, we maintained the reduction and confirmed the excellent position of the wire in the distal femur. A 360-mm carbon fiber nail with an 11-mm diameter was measured. We sequentially reamed up to size 12.5 mm, and smoothly inserted using a tube exchanger to remove the ball tip guidewire and insert the smooth one. The carbon fiber femoral nail was inserted over the smooth wire in the traditional fashion, with the aiming arm positioned anteriorly, externally rotating the aiming arm as the nail is advanced. The rod is tapped to its final position until the top part of the rod is covered by the proximal femur.
Manipulating the soft tissues, we utilized the incision from the biopsy to insert the triple trochar through the aiming arm. We then inserted through the femoral guidewire for the trajectory in the femoral neck for the hip screw. Under fluoroscopy, proper position was confirmed. Reaming to a length of 95 mm was achieved. The instrument for the hip screw was secured without difficulty, initially tapping the path and then inserting the screw following the marked trajectory in the femoral neck, and then securing it with the setting screw.
Maintaining a perfect AP of the right hip and knee, the distal portion of the nail was secured with two 5.0-mm titanium screws measuring 40 and 40.5 mm in length (Figure 4). Final images confirmed successful reduction of the fracture and optimal hardware positioning (Figure 5). Copious irrigation was performed, followed by layer-by-layer closure. There were no complications during the case. The case length was 121 minutes with an estimated blood loss of 250 mL.
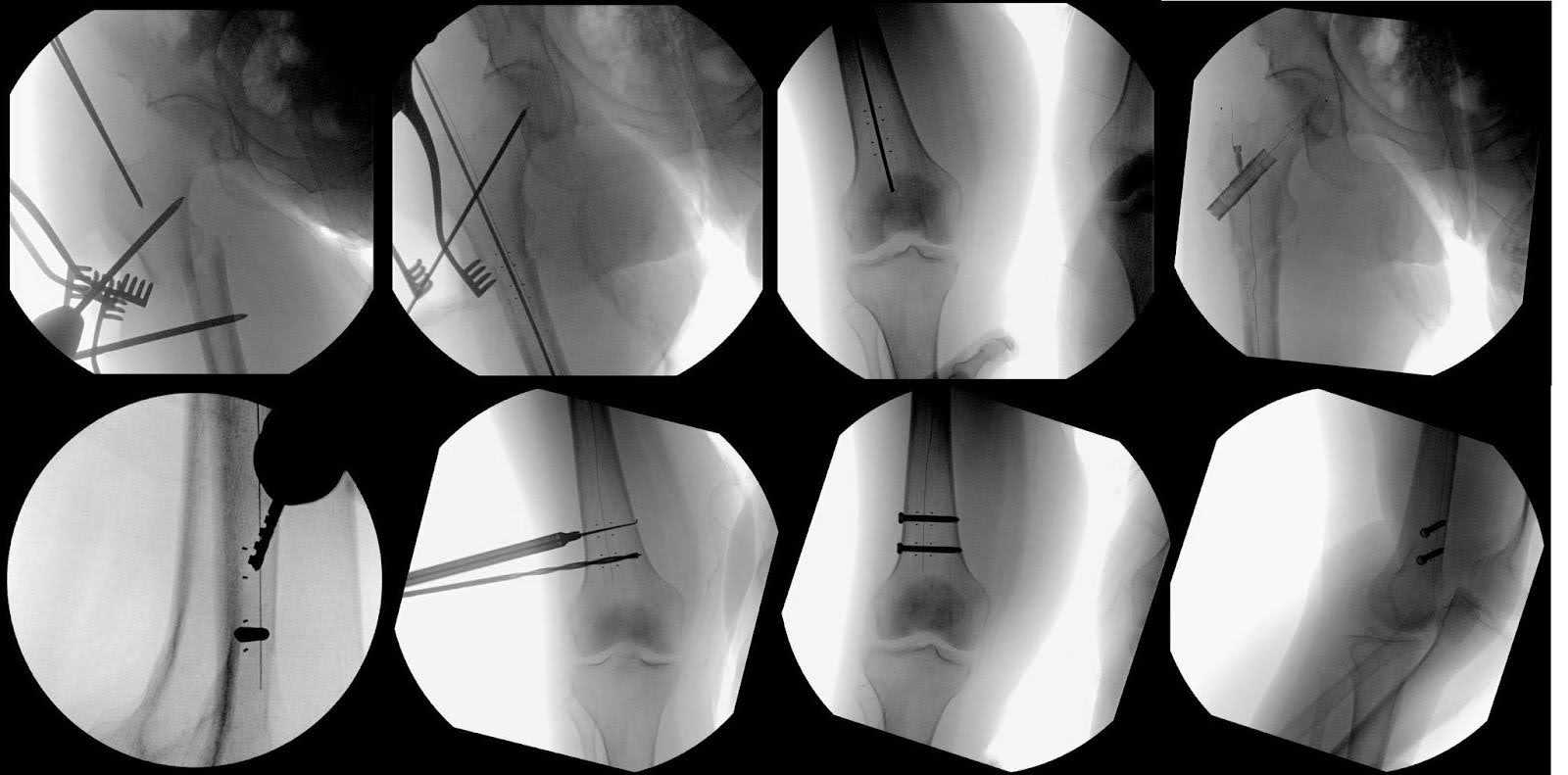
Figure 4. Fluoroscopy imaging was used to demonstrate the different surgical steps involved in treating the femur fracture. This included showing the starting point and reduction of the fracture using Shantz pins. Additional imaging was used to show the carbon fiber nail, carbon fiber hip screw, and two titanium interlocking screws that were used to ensure the stability of the nail. Radio-opaque markers aided in visualizing these apertures, observable from both AP and lateral views. It is noteworthy that the guides for these entry holes differ from the standard circular ones typically visible in fluoroscopy for titanium nails.

Figure 5. An AP x-ray of the femur and a lateral x-ray of the knee post carbon fiber intramedullary rod fixation for a pathologic subtrochanteric fracture of the right femur show improved alignment with no signs of hardware complications. The lower leg reveals no additional suspicious lytic lesions, and there is no indication of new fractures.
Discussion
An open biopsy of the right proximal femur was performed in addition to operative fixation, and a 5.5x5.5x2.5-cm specimen, consisting of dusty pink-red soft tissue fragments, was sent for histopathological assessment by a fellowship-trained bone and soft tissue pathologist. An immunostain for PD-L1 was performed on a representative tissue block and revealed >100 tumor cells available for scoring. PD-L1 showed membranous staining of strong intensity in >95% of tumor cells (tumor proportion score, or TPS, >95%).25 Immunohistochemistry showed tumor cells that were positive for TTF-1 and Napsin-A and negative for p40. Given these findings, the final pathologic diagnosis of the right proximal femur lesion is metastatic carcinoma consistent with lung primary.26–28
One month after surgery, the patient received 20 Gy of palliative radiation in five fractions to the right hip. In the setting of metastatic bone disease, radiation therapy mitigates osteoclast activation, kills tumor cells, and alleviates bone pain by producing ossification.29 Concurrently, medical oncology started the patient on Capmatinib, a targeted therapy used to treat metastatic non-small cell lung cancer. At the two-month follow-up, the patient demonstrated substantial improvement, being able to ambulate without a walker. Her knees were stable to valgus and varus stress on full extension and 30° of flexion. Hip flexion, extension, internal rotation, and external rotation were within normal limits. By six weeks after starting Capmatinib, the patient was responding well to treatment. A CT of the chest showed a decreased mass in the right upper lobe and decreased bilateral mediastinal and hilar lymphadenopathy. At her most recent follow-up, her functional status has shown no significant changes with no discernable hardware changes, and she continues to receive Capmatinib, undergoing frequent radiographic monitoring (Figure 7).

Figure 6. AP and lateral x-rays of the femur and a lateral x-ray of the knee, two months after fixation, show new callus formation and bony bridging, maintaining original alignment. No new fractures are present, but mild degenerative changes observed in the right hip.
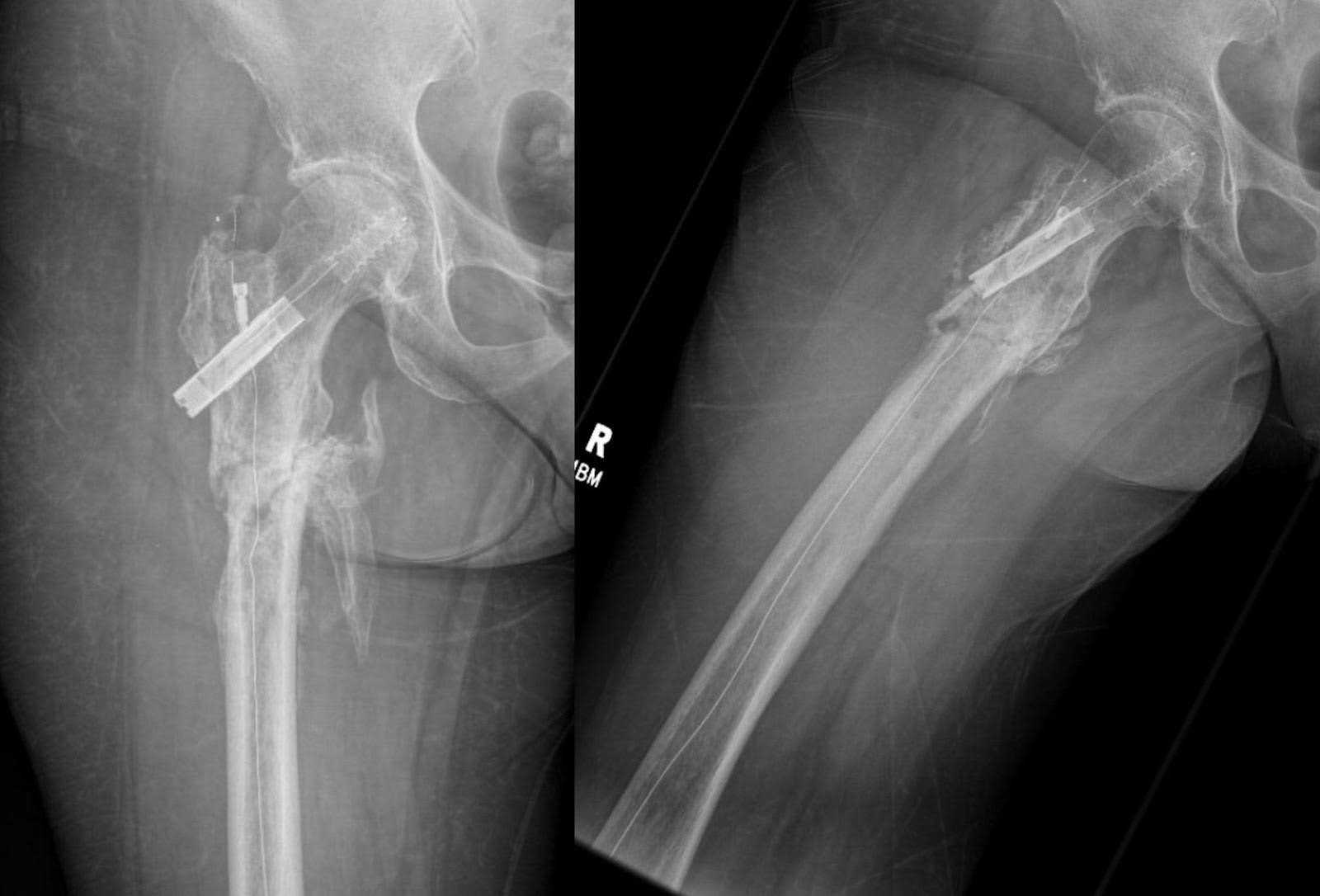
Figure 7. At six months after fixation, AP and lateral femur x-rays reveal continued callus formation and copious bony bridging, maintaining the initial alignment. The fracture displays signs of incomplete healing alongside the presence of heterotopic bone formation. There are no discernible hardware complications or indications of new fractures. Furthermore, analogous degenerative changes persist in the right hip.
Metastasis plays a significant role in the morbidity and mortality associated with cancer.30 Lung cancer, the second most common carcinoma in men and women, respectively, exhibits a preference for metastasis in the brain, bones, and adrenal glands.31,32 Metastatic bone disease not only inflicts debilitating pain on patients but also imposes a substantial financial burden. The current estimate of 250,000 patients in the United States grappling with this condition translates to an annual healthcare cost of $12 billion.33,34 Advances in treatments, while improving cancer survival rates, have consequently led to a higher incidence of metastatic bone disease. Pathologic fractures arising from this condition stem from numerous lesions reaching a size that jeopardizes the structural integrity of the bone, ultimately culminating in fractures.35 To improve long-term patient survival and quality of life, it is crucial to prioritize appropriate treatment modalities in disease management strategically.36
As this patient carried no oncologic diagnosis prior to the femur fracture, it is important to highlight the key points that can help identify at risk bony lesions prior to fracture. The patient reported multiple months of pain in the hip prior to the fracture, which can often be the first clinical finding of any visceral carcinoma. Shrewd history taking and physical exam findings that reveal pain that has no explanation, especially functional pain should be investigated. The most appropriate method of evaluation is with plain radiographs of the entire bone in the extremity that is affected, to ensure that referred pain is not a masking clinical factor.
After the fracture is treated appropriately and the patient has survived the immediate postoperative phase, attention must turn to addressing the underlying disease, necessitating a multidisciplinary approach involving medical and radiation oncology. Medical oncology provides systemic treatment for both the primary cancer and its metastatic lesions. Radiation oncology serves a critical purpose in local treatment within the subacute postoperative period, aggressively targeting disseminated cancer cells to facilitate the essential bony healing process. Although case series report a lower rate of disease progression after medullary nail stabilization, the risk of hardware failure increases with patient survival.37,38 Carbon fiber implants can improve disease monitoring and bone healing when used with advanced imaging techniques.12 Studies investigating patient-reported outcomes and cost-effectiveness of carbon fiber implants versus titanium may enhance clinical adoption.
Equipment
No special equipment used beyond the carbon fiber implant.
Disclosures
The corresponding author is a paid speaker and consultant for CarboFix Orthopaedics Ltd.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Note
Animation added post-publication on 10/03/2025. No changes were made to the article content.
Citations
- Haase SC. Treatment of pathologic fractures. Hand Clin. 2013;29(4):579-584. doi:10.1016/j.hcl.2013.08.010.
- Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12(20 Pt 2):6243s-6249s. doi:10.1158/1078-0432.CCR-06-0931.
- Hage WD, Aboulafia AJ, Aboulafia DM. Incidence, location, and diagnostic evaluation of metastatic bone disease. Orthop Clin North Am. 2000;31(4):515-528, vii. doi:10.1016/s0030-5898(05)70171-1.
- Christ AB, Piple AS, Gettleman BS, et al. Prevalence of primary malignant tumours, rates of pathological fracture, and mortality in the setting of metastatic bone disease. Bone Jt Open. 2023;4(6):424-431. doi:10.1302/2633-1462.46.BJO-2023-0042.R1.
- Johnson SK, Knobf MT. Surgical interventions for cancer patients with impending or actual pathologic fractures. Orthop Nurs. 2008;27(3):160-171; quiz 172-173. doi:10.1097/01.NOR.0000320543.90115.d5.
- De Mattos CBR, Binitie O, Dormans JP. Pathological fractures in children. Bone Joint Res. 2012;1(10):272-280. doi:10.1302/2046-3758.110.2000120.
- Kim LD, Bueno FT, Yonamine ES, Próspero JD de, Pozzan G. Bone metastasis as the first symptom of tumors: role of an immunohistochemistry study in establishing primary tumor. Rev Bras Ortop (Sao Paulo). 2018;53(4):467-471. doi:10.1016/j.rboe.2018.05.015.
- Yoon RS, Donegan DJ, Liporace FA. Reducing subtrochanteric femur fractures: tips and tricks, do’s and don’ts. J Orthop Trauma. 2015;29 Suppl 4:S28-33. doi:10.1097/BOT.0000000000000287.
- Weiss RJ, Ekström W, Hansen BH, et al. Pathological subtrochanteric fractures in 194 patients: a comparison of outcome after surgical treatment of pathological and non-pathological fractures. J Surg Oncol. 2013;107(5):498-504. doi:10.1002/jso.23277.
- Depauw N, Pursley J, Lozano-Calderon SA, Patel CG. Evaluation of carbon fiber and titanium surgical implants for proton and photon therapy. Pract Radiat Oncol. 2023;13(3):256-262. doi:10.1016/j.prro.2023.01.009.
- Lozano-Calderon SA, Rijs Z, Groot OQ, et al. Outcomes of long bones treated with carbon-fiber nails for oncologic indications: international multi-institutional study. J Am Acad Orthop Surg. 2024;32(3):e134-e145. doi:10.5435/JAAOS-D-22-01159.
- Yeung CM, Bhashyam AR, Groot OQ, et al. Comparison of carbon fibre and titanium intramedullary nails in orthopaedic oncology. Bone Jt Open. 2022;3(8):648-655. doi:10.1302/2633-1462.38.BJO-2022-0092.R1.
- Ernstberger T, Heidrich G, Bruening T, Krefft S, Buchhorn G, Klinger HM. The interobserver-validated relevance of intervertebral spacer materials in MRI artifacting. Eur Spine J. 2007;16(2):179-185. doi:10.1007/s00586-006-0064-5.
- Alvarez-Breckenridge C, de Almeida R, Haider A, et al. Carbon fiber-reinforced polyetheretherketone spinal implants for treatment of spinal tumors: perceived advantages and limitations. Neurospine. 2023;20(1):317-326. doi:10.14245/ns.2244920.460.
- Clunk MJ, Gonzalez MR, Denwood HM, et al. A PEEK into carbon fiber: a practical guide for high performance composite polymeric implants for orthopaedic oncology. J Orthop. 2023;45:13-18. doi:10.1016/j.jor.2023.09.011.
- Manglani HH, Marco RA, Picciolo A, Healey JH. Orthopedic emergencies in cancer patients. Semin Oncol. 2000;27(3):299-310.
- Booth K, Rivet J, Flici R, et al. Progressive mobility protocol reduces venous thromboembolism rate in trauma intensive care patients: a quality improvement project. J Trauma Nurs. 2016;23(5):284-289. doi:10.1097/JTN.0000000000000234.
- Colyer RA. Surgical stabilization of pathological neoplastic fractures. Curr Probl Cancer. 1986;10(3):117-168. doi:10.1016/s0147-0272(86)80005-8.
- Xin-ye N, Xiao-bin T, Chang-ran G, Da C. The prospect of carbon fiber implants in radiotherapy. J Appl Clin Med Phys. 2012;13(4):3821. doi:10.1120/jacmp.v13i4.3821.
- Bhashyam AR, Yeung C, Sodhi A, et al. Titanium vs. carbon fiber-reinforced intramedullary nailing for humeral bone tumors. J Shoulder Elbow Surg. 2023;32(11):2286-2295. doi:10.1016/j.jse.2023.04.023.
- Cofano F, Di Perna G, Monticelli M, et al. Carbon fiber reinforced vs titanium implants for fixation in spinal metastases: a comparative clinical study about safety and effectiveness of the new “carbon-strategy”. J Clin Neurosci. 2020;75:106-111. doi:10.1016/j.jocn.2020.03.013.
- Yeung CM, Bhashyam AR, Patel SS, Ortiz-Cruz E, Lozano-Calderón SA. Carbon fiber implants in orthopaedic oncology. J Clin Med. 2022;11(17). doi:10.3390/jcm11174959.
- Tedesco G, Gasbarrini A, Bandiera S, Ghermandi R, Boriani S. Composite PEEK/carbon fiber implants can increase the effectiveness of radiotherapy in the management of spine tumors. J Spine Surg. 2017;3(3):323-329. doi:10.21037/jss.2017.06.20.
- Nevelsky A, Borzov E, Daniel S, Bar-Deroma R. Perturbation effects of the carbon fiber-PEEK screws on radiotherapy dose distribution. J Appl Clin Med Phys. 2017;18(2):62-68. doi:10.1002/acm2.12046.
- Keppens C, Dequeker EM, Pauwels P, Ryska A, ’t Hart N, von der Thüsen JH. PD-L1 immunohistochemistry in non-small-cell lung cancer: unraveling differences in staining concordance and interpretation. Virchows Arch. 2021;478(5):827-839. doi:10.1007/s00428-020-02976-5.
- Yatabe Y, Mitsudomi T, Takahashi T. TTF-1 expression in pulmonary adenocarcinomas. Am J Surg Pathol. 2002;26(6):767-773. doi:10.1097/00000478-200206000-00010.
- Zhang P, Han YP, Huang L, Li Q, Ma DL. Value of napsin A and thyroid transcription factor-1 in the identification of primary lung adenocarcinoma. Oncol Lett. 2010;1(5):899-903. doi:10.3892/ol_00000160.
- Affandi KA, Tizen NMS, Mustangin M, Zin RRMRM. p40 immunohistochemistry is an excellent marker in primary lung squamous cell carcinoma. J Pathol Transl Med. 2018;52(5):283-289. doi:10.4132/jptm.2018.08.14.
- De Felice F, Piccioli A, Musio D, Tombolini V. The role of radiation therapy in bone metastases management. Oncotarget. 2017;8(15):25691-25699. doi:10.18632/oncotarget.14823.
- Nooh A, Goulding K, Isler MH, et al. Early improvement in pain and functional outcome but not quality of life after surgery for metastatic long bone disease. Clin Orthop Relat Res. 2018;476(3):535-545. doi:10.1007/s11999.0000000000000065.
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763.
- Popper HH. Progression and metastasis of lung cancer. Cancer Metastasis Rev. 2016;35(1):75-91. doi:10.1007/s10555-016-9618-0.
- Guy GP, Ekwueme DU, Yabroff KR, et al. Economic burden of cancer survivorship among adults in the United States. J Clin Oncol. 2013;31(30):3749-3757. doi:10.1200/JCO.2013.49.1241.
- Li S, Peng Y, Weinhandl ED, et al. Estimated number of prevalent cases of metastatic bone disease in the US adult population. Clin Epidemiol. 2012;4:87-93. doi:10.2147/CLEP.S28339.
- Blank AT, Lerman DM, Patel NM, Rapp TB. Is prophylactic intervention more cost-effective than the treatment of pathologic fractures in metastatic bone disease? Clin Orthop Relat Res. 2016;474(7):1563-1570. doi:10.1007/s11999-016-4739-x.
- Gutowski CJ, Zmistowski B, Fabbri N, Boland PJ, Healey JH. Should the use of biologic agents in patients with renal and lung cancer affect our surgical management of femoral metastases? Clin Orthop Relat Res. 2019;477(4):707-714. doi:10.1097/CORR.0000000000000434.
- Miller BJ, Soni EEC, Gibbs CP, Scarborough MT. Intramedullary nails for long bone metastases: why do they fail? Orthopedics. 2011;34(4). doi:10.3928/01477447-20110228-12.
- Arpornsuksant P, Morris CD, Forsberg JA, Levin AS. What factors are associated with local metastatic lesion progression after intramedullary nail stabilization? Clin Orthop Relat Res. 2022;480(5):932-945. doi:10.1097/CORR.0000000000002104.



| Publication Date | 5/23/2024 |
| Article ID | 443 |
| Production ID | 0443 |
| Volume | 2024 |
| Issue | 443 |
| DOI | |
| https://doi.org/10.24296/jomi/443 | |