The Use of a Magnetic Intramedullary Nail for Management of a Symptomatic Nonunion Following Shortening Osteotomy to Treat Leg-Length Discrepancy
Abstract
We present the case of a 31-year-old female with a history of juvenile rheumatoid arthritis and uveitis who presented to our department with a leg-length discrepancy and low back pain refractory to conservative management. She underwent a shortening osteotomy on her left femur around an intramedullary nail that went on to nonunion. She underwent exchange nailing with a magnetic intramedullary nailing with autologous bone graft harvest from her affected femoral reamings. The magnetic intramedullary nail was extended 2 cm prior to insertion, and then implanted in the usual fashion with immediate compression in the operating room. Postoperatively the patient underwent a compressive program using the magnetic nail and went on to heal her osteotomy site.
Keywords
Nonunion; limb-length discrepancy; limb lengthening.
Case Overview
Background
Limb-length discrepancy (LLD) is common, with estimates of prevalence ranging from 40–90% of the population.1,2 Nonoperative management is indicated for patients with LLD of 0–2cm, while those with larger discrepancies or continued symptoms after conservative management can benefit from surgical intervention.3,4 Surgery can consist of either shortening or lengthening and can be stabilized with an intramedullary implant or extramedullary fixation. Additionally, magnetic devices have been introduced for both bone transport in limb salvage or in LLD in pediatric and adult populations.5 There is a risk of complications with surgical intervention of up to 34% in patients undergoing shortening procedure for nonunion or malunion.6 The patient in our care underwent an initial shortening osteotomy around a static intramedullary implant that corrected her LLD but went on to a painful nonunion. After discussion with the patient, the plan was for exchange nailing with a magnetic intramedullary implant and local autologous bone graft to heal her nonunion.
Focused History of the Patient
Our patient was a 31-year-old woman with a history of juvenile rheumatoid arthritis (JRA) with uveitis who presented with a 17-mm LLD (left longer than right) focused on the femur causing low back pain. She had a growth arrest procedure performed on her left knee as a child and continued to have symptoms related to her LLD. She had done physical therapy and had two SI joint injections with corticosteroid and local anesthetic, which did not provide durable relief. She was evaluated in the office and standing films confirmed her LLD. She was given a shoe lift, and she trialed this for 7 weeks. However, she was unable to fit the shoe lift into her typical footwear and did not want to wear an external shoe lift and was interested in surgery. She saw her rheumatologist as she was on an infusion of infliximab every 6 weeks for her JRA and agreed to stop the medication in the perioperative period. Preoperatively her BMI was 33.7, she was an American Society of Anaesthesiologist (ASA) score III, and she was a nonsmoker. The risk of nonunion given her immunotherapy was discussed.
The patient presented for surgical management with a shortening osteotomy of the left femur around an intramedullary nail. She was supine on a fracture table for the procedure and had a 9x380-mm trochanteric entry nail inserted in the usual fashion. After the nail was inserted, a subvastus approach was made to the femur with an 18-mm osteotomy completed using a 2.5 drill for pilot holes and a sagittal saw to complete the osteotomy. Electrocautery was used to mark the version on the femur prior to completing the osteotomy. Two screws were fixed proximally, one recon screw in the femoral neck, and one in the lesser trochanter. Two screws, one static and one dynamic were placed in the distal interlocks. Her wound was closed in layers with 1 g of Vancomycin powder placed deep. Her estimated blood loss (EBL) was 100 ml, and the operative time was 238 minutes. Postoperatively she was weightbearing as tolerated and discharged to home on postoperative day 4.
At her first postoperative visit 3 weeks later her wounds were healing well. Unfortunately, she did develop labial pressure wounds after being on the fracture table, which were treated conservatively by gynecology. The plan at that time was to hold her Infliximab infusion for a total of 7–9 weeks postoperatively; however, she had a uveitis flare and needed to resume her infusions earlier. At her next follow up 3 months postoperatively, standing films confirmed that her pelvic tilt and LLD had resolved; however, she was still walking with a walker and had not been able to wean to a crutch secondary to pain. She was seen again 5 months postoperatively with concern for a nonunion, was encouraged to continue a home exercise program and was given a bone stimulator. Nonunion labs at that time were notable for WBC 6.7, ESR 6, 25(OH) Vitamin D of 23, TSH 0.96, PTH 34, Albumin 4.1. Unfortunately, by 6 months she still had pain and no further healing and was indicated for exchange nailing with autologous bone grafting.
She was taken back to the operating room 9.5 months following her index procedure for hardware removal and exchange nailing. She was placed in lateral decubitus with a bean bag positioner. Her hardware was removed using her prior incisions. The osteotomy site was revised with a 3.5 drill making a single lateral hole with multiple medial holes to facilitate autologous bone graft retention. The femur was reamed up to 14 mm, and autologous bone graft was seen depositing on the medial side fluoroscopically and placed on the lateral side of the femur. The osteotomy was completed using an osteotome. A magnetic NuVasive Precice rod was used after being extended 2 cm on the back table prior to insertion. Once the nail was in place, Judet decortication was performed on the lateral femur and reamings were deposited laterally. The wound was closed in layers and sterile dressings placed. Operative time was 233 minutes, and EBL was 500 cc. The patient was touchdown weight bearing postoperatively and was discharged on postoperative day 2.
The patient was seen two weeks postoperatively and her incisions were well-healing, she had a shortening in the office and maintained touchdown weight bearing. This was repeated for two weeks, and she was made weightbearing as tolerated on postoperative week 6. Her immunosuppressives were resumed 4 months postoperatively once bridging callus was seen. At 6 months postoperatively, her osteotomy site had healed, she had improvements in her pain and gait, and she was referred to spine for persistent lumbar back pain. At her most recent follow up 9 months postoperatively, she had weaned from ambulatory aids for short distances, her back pain and leg pain had improved, and she was considering elective hardware removal.
Physical Exam
On exam the patient was well-appearing, with pain at the SI joints bilaterally and a 17-mm LLD (left longer than right) confirmed on block testing and standing films. There were no skin changes over the left leg, and she was neurovascularly intact distally.
Imaging
Imaging results for this patient can be seen in Figures 1–3.
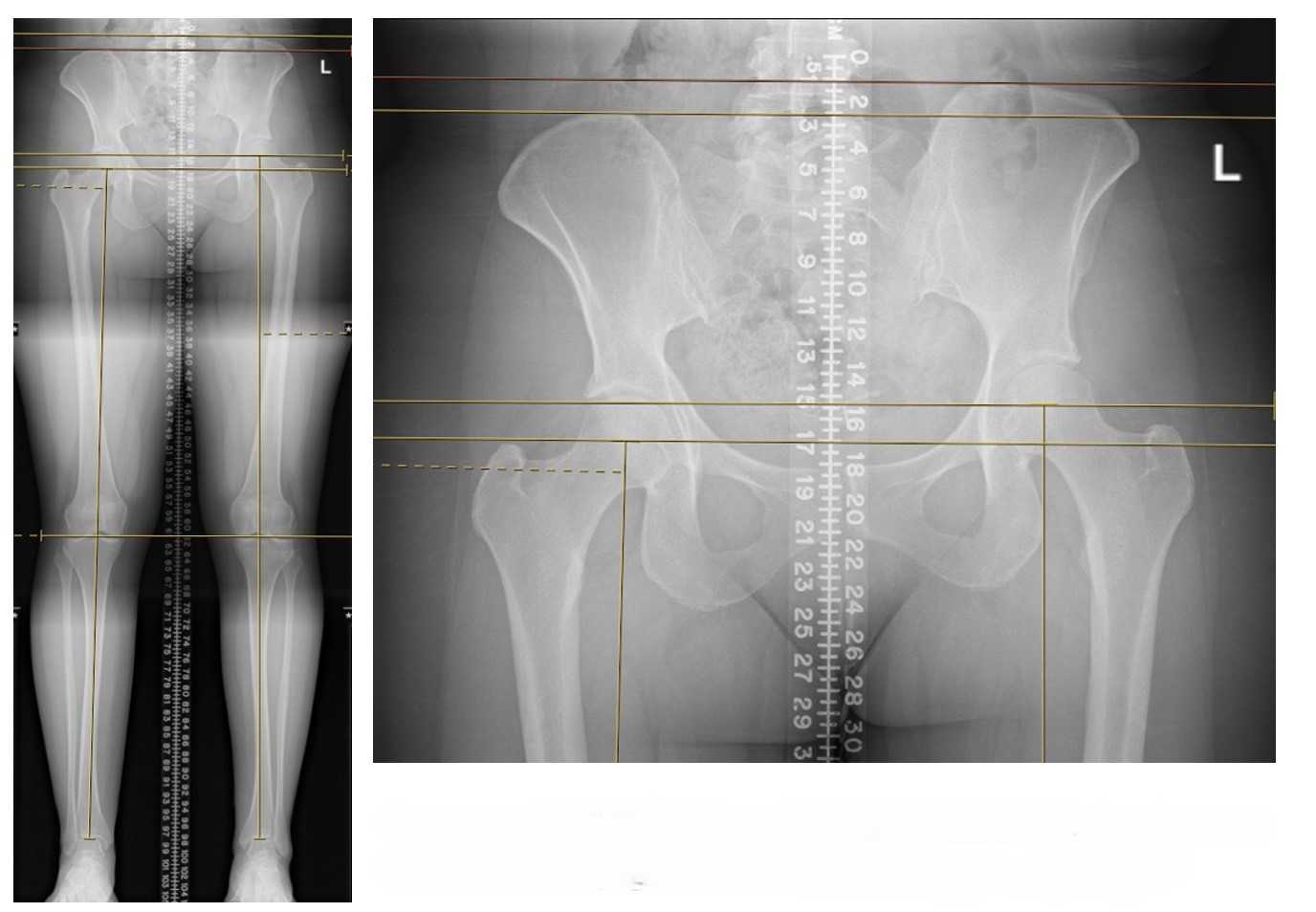
Figure 1. Presentation images with a 17-mm leg-length discrepancy (right shorter than left), from femur.

Figure 2. Three months postoperative standing films with correction of leg-length discrepancy but persistent pain, requiring walker for ambulation.
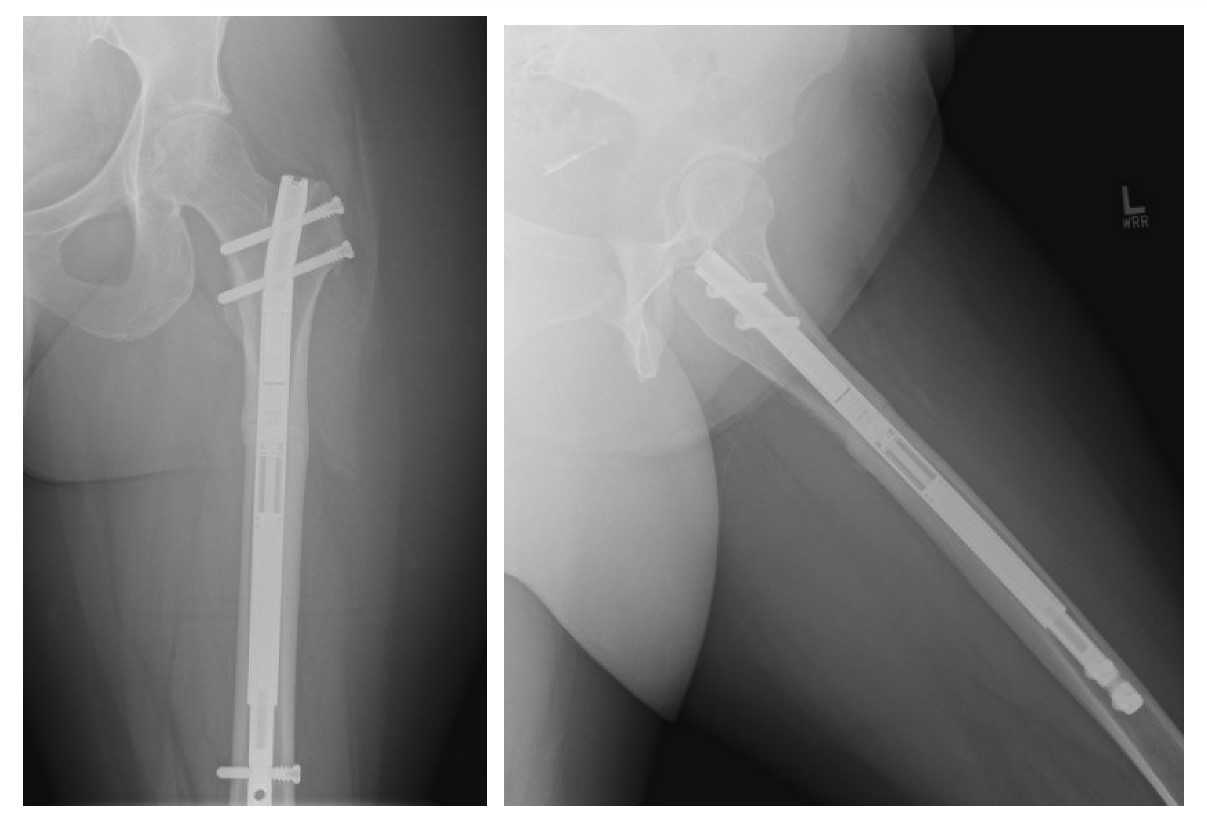
Figure 3. Most recent follow up, 9 months after surgery. Able to walk short distances without assistive devices, and considering implant removal after 1 year.
Natural History
LLD is a common problem, with one study by Gordon et al suggesting that only 10% of 573 patients studied had exactly equal leg lengths, while one paper by Gurney et al. quoted a 40–70% prevalence of LLD in the US population.1,2 Specific to the population of patients with JRA, one historic paper by Simon et al. quoted that of 51 patients with follow up over 4 years in 1981 all had a measurable LLD, with 70% having a LLD over 1.5 cm.7 Prior studies have suggested that a LLD over 2 cm may be associated with hip, knee, and spine osteoarthritis, and this has been used as an indication for surgery.1,8
Options for Treatment
First-line treatment for LLD is nonoperative management, as differences of up to 2 cm are generally accepted to be well-tolerated without intervention. These can be managed with shoe lifts which can either be inserted into regular footwear or in the form of custom-manufactured shoes with height built-in. Surgical management in the adult patient with closed physes involves either a shortening osteotomy or a lengthening or bone transport. Shortening may be pursued for relatively small LLD, while for larger differences such as after trauma or infection, lengthening may be preferred.4 Shortening osteotomies can be done over an intramedullary device or can be performed with stabilization using plate osteosynthesis. Lengthening can be done over standard intramedullary nails, magnetic nails, or ringed fixators.
Rationale for Treatment
The goal of treatment is to reduce pain and improve function in the short term, and to possibly prevent further sequelae of hip, knee, or spinal degenerative changes in the long term.
Special Considerations
Patients who have symptomatic LLD, whether after congenital or pediatric acquired conditions as in our patient, or after trauma or infection, can be indicated for surgical correction of LLD.
Discussion
We present the case of a 31-year-old patient with a history of JRA who had a 17-mm LLD (left longer than right), which was refractory to nonoperative treatment including physical therapy and shoe lifts and who sought surgical intervention. She was taken to the operating room for a shortening osteotomy of her left femur over a static trochanteric entry nail. She was supine on a fracture table for a total of 238 minutes with 100 cc EBL. Unfortunately, she developed labial pressure wounds from the time on the traction table that were managed nonoperatively. She required return to the operating room 9.5 months after her index procedure due to a painful nonunion across her osteotomy site. She underwent exchange nailing with a magnetic implant which was done in the lateral decubitus position with an operative time of 233 minutes and EBL of 500 cc. After a period of touchdown weight bearing for 6 weeks, she was made weightbearing as tolerated and went on to heal her nonunion by 6 months after her exchange nailing. Her incisions healed well, and her pain was improved compared to before her procedures, although she still had some symptomatic low back pain.
This case demonstrates some of the challenges of managing LLD in patients. While patients with LLD of <2 cm may be managed nonoperatively, patients with discrepancies of 4–6 cm may be managed with shortening procedures on the longer limb, and patients with greater than 6 cm of discrepancy may benefit from a combination of lengthening the shorter limb and or shortening the longer limb.4 While patients with open physes may use growth arrest at the physis to induce relative shortening, adults with closed physes necessitate an osteotomy for shortening.3 The use of external fixators to lengthen bone via distraction osteogenesis was pioneered by Ilizarov, but later intramedullary devices were introduced as a tool for lengthening, with the advantages of shortened time for lengthening, avoidance of pin tract infections, and maintaining the angular alignment and avoiding fracture after frame removal.9–11 Motorized driven nails which are able to transport bone without the use of external fixators have been used in limb lengthening, with some positive results but a not insignificant complication rate.5,12–14
The management of nonunions remains a challenge in orthopaedics, with traditional teaching dividing nonunions into atrophic nonunions thought to be a problem of biology, hypertrophic nonunion thought to be due to lack of stability, and oligotrophic nonunions with intermediate features. Our patient presented with an atrophic nonunion without obvious laboratory abnormalities. One contributing factor possibly relating to nonunion in this case was the use of her immunologic therapy. While DMARD medications such as infliximab are recommended to be held 5–9 weeks preoperatively in patients undergoing primary total joint arthroplasty, there do not exist clear guidelines regarding the timing of the use of these medications for lengthening or shortening osteotomies.15 While the patient’s rheumatologist was involved in determining an appropriate time to be off her biologic therapy, a uveitis flare necessitated starting the therapy again.
Without modifiable systemic biologic factors, surgical management was planned with exchange nailing and compression. Different options exist for managing nonunion in the femur, from exchange nailing alone compared to compression plating or a combination of the two.16–18 Recently motorized driven nails have been used to provide dynamic compression across a nonunion site, with high rates of union but not insignificant complication profile.6,19 This case highlights an emerging use of motorized intramedullary nailing for management of nonunions following limb-lengthening surgery. Our patient went onto heal her nonunion but still had symptomatic low back pain, highlighting the importance of counseling patients on the risks and benefits of operative vs. nonoperative management of this common condition. Further research is needed to better determine the ideal treatment algorithm for these patients, as well as the timing of immunologic therapy in patients in fracture or nonunion surgery.
Equipment
- Precice nail, Nuvasive.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Citations
- Gordon JE, Davis LE. Leg length discrepancy: the natural history (and what do we really know). J Pediatr Orthop. 2019;39(6):S10-S13. doi:10.1097/BPO.0000000000001396.
- Gurney B, Mermier C, Robergs R, Gibson A, Rivero D. Effects of limb-length discrepancy on gait economy and lower-extremity muscle activity in older adults. J Bone Jt Surg. 2001;83(6):907-915. doi:10.2106/00004623-200106000-00013.
- Hubbard EW, Liu RW, Iobst CA. Understanding skeletal growth and predicting limb-length inequality in pediatric patients. J Am Acad Orthop Surg. 2019;27(9):312-319. doi:10.5435/JAAOS-D-18-00143.
- Stanitski DF. Limb-length inequality: assessment and treatment options. J Am Acad Orthop Surg. 1999;7(3):143-153. doi:10.5435/00124635-199905000-00001.
- Frommer A, Roedl R, Gosheger G, et al. What are the potential benefits and risks of using magnetically driven antegrade intramedullary lengthening nails for femoral lengthening to treat leg length discrepancy? Clin Orthop Relat Res. 2022;480(4):790-803. doi:10.1097/CORR.0000000000002036.
- Zuluaga M, Pérsico F, Medina J, Reina F, Jiménez N, Benedetti F. Precice nail for the management of posttraumatic bone defects with nonunion or malunion: experience from a Latin American center. Injury. 2023;54(May). doi:10.1016/j.injury.2023.110838.
- Simon S, Whiffen J, Shapiro F. Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Jt Surg - Ser A. 1981;63(2):209-215. doi:10.2106/00004623-198163020-00005.
- Subotnick SI. Limb length discrepancies of the lower extremity (the short leg syndrome). J Orthop Sports Phys Ther. 1981;3(1):11-16. doi:10.2519/jospt.1981.3.1.11.
- Calder PR, Wright J, Goodier WD. An update on the intramedullary implant in limb lengthening: a quinquennial review part 2: extending surgical indications and further innovation. Injury. 2022;53:S88-S94. doi:10.1016/j.injury.2022.06.024.
- Calder PR, Wright J, Goodier WD. An update on the intramedullary implant in limb lengthening: a quinquennial review Part 1: the further influence of the intramedullary nail in limb lengthening. Injury. 2022;53:S81-S87. doi:10.1016/j.injury.2022.06.028.
- Hosny GA. Limb lengthening history, evolution, complications and current concepts. J Orthop Traumatol. 2020;21(1). doi:10.1186/s10195-019-0541-3.
- Frost MW, Rahbek O, Traerup J, Ceccotti AA, Kold S. Systematic review of complications with externally controlled motorized intramedullary bone lengthening nails (Fitbone and Precice) in 983 segments. Acta Orthop. 2020;92(1):120-127. doi:10.1080/17453674.2020.1835321.
- Hammouda AI, Jauregui JJ, Gesheff MG, Standard SC, Conway JD, Herzenberg JE. Treatment of post-traumatic femoral discrepancy with Precice magnetic-powered intramedullary lengthening nails. J Orthop Trauma. 2017;31(7):369-374. doi:10.1097/BOT.0000000000000828.
- Wiebking U, Liodakis E, Kenawey M, Krettek C. Limb lengthening using the Precice nail system: complications and results. Arch Trauma Res. 2016;5(4). doi:10.5812/atr.36273.
- Goodman SM, Springer BD, Chen AF, et al. 2022 American College of Rheumatology/American Association of Hip and Knee Surgeons Guideline for the Perioperative Management of Antirheumatic Medication in Patients With Rheumatic Diseases Undergoing Elective Total Hip or Total Knee Arthroplasty. Arthritis Care Res. 2022;74(9):1399-1408. doi:10.1002/acr.24893.
- Marquez-Lara A, David Luo T, Senehi R, Aneja A, Beard HR, Carroll EA. Exchange nailing for hypertrophic femoral nonunion. J Orthop Trauma. 2017;31(8):S23-S25. doi:10.1097/BOT.0000000000000905.
- Brinker MR, O’Connor DP. Management of aseptic tibial and femoral diaphyseal nonunions without bony defects. Orthop Clin North Am. 2016;47(1):67-75. doi:10.1016/j.ocl.2015.08.009.
- Lynch JR, Taitsman LA, Barei DP, Nork SE. Femoral nonunion: risk factors and treatment options. J Am Acad Orthop Surg. 2008;16(2):88-97. doi:10.5435/00124635-200802000-00006.
- Fragomen AT, Wellman D, Rozbruch SR. The Precice magnetic IM compression nail for long bone nonunions: a preliminary report. Arch Orthop Trauma Surg. 2019;139(11):1551-1560. doi:10.1007/s00402-019-03225-4.


| Publication Date | 8/16/2024 |
| Article ID | 446 |
| Production ID | 0446 |
| Volume | 2024 |
| Issue | 446 |
| DOI | |
| https://doi.org/10.24296/jomi/446 | |