Laparoscopic Appendectomy with Lysis of Adhesions for Appendicitis
Abstract
This video demonstrates a laparoscopic appendectomy with lysis of adhesions in a patient with prior umbilical hernia repair. Modified port placement was used to avoid encountering known adhesions from previous surgery. Intraoperatively, additional adhesions were lysed to allow safe access to the inflamed appendix. The mesoappendix was divided with a bipolar energy device, and the appendix was resected using a 45-mm stapler. The staple line was reinforced, the field irrigated, and the specimen retrieved. This case highlights practical strategies for navigating adhesions during laparoscopic appendectomy.
Case Overview
Laparoscopic appendectomy (LA) has been widely adopted as the standard surgical approach for the treatment of acute appendicitis since its introduction in the 1980s.1 This minimally-invasive technique is distinguished by the utilization of small incisions through which an endoscopic camera and specialized instruments are introduced to facilitate the excision of the inflamed vermiform appendix. The benefits of LA over open surgery have been well documented in the literature, including reduced postoperative pain, shorter hospital stays, and faster return to normal activities.2,3
In some cases, particularly in patients with a history of abdominal surgeries, adhesions may be encountered during the procedure.4,5 These fibrous bands of scar tissue can complicate access to the appendix and necessitate additional steps in the surgery, known as lysis of adhesions.6 The combination of LA with lysis of adhesions requires advanced laparoscopic skills and may prolong operative time.
The LA with lysis of adhesions is performed through a series of carefully executed steps, as demonstrated in this video.
The procedure begins with identifying Palmer’s point for Veress needle insertion, located in the left upper quadrant, approximately 2–3 cm below the costal margin in the midclavicular line. After Veress needle insertion, the abdomen is insufflated with carbon dioxide to establish pneumoperitoneum. Due to the patient’s history of umbilical hernia repair, a modified approach is used: an optical 12-mm trocar is initially inserted supraumbilically to avoid the previous umbilical repair site. Upon entering the abdominal cavity, adhesions—likely from the previous repair—are encountered, partially trapping the 12-mm trocar. Subsequently, three additional ports are placed in the left lower quadrant (Figure 1), suprapubic region, and right lower quadrant, respectively. A 5-mm scope is mounted on the camera and introduced via the left lower quadrant port. Adhesions are then lysed using a combination of sharp and blunt dissection, carefully separating them from the abdominal wall to avoid injuring underlying structures. This step is essential for accessing the appendix and achieving a clear view of the surgical field.
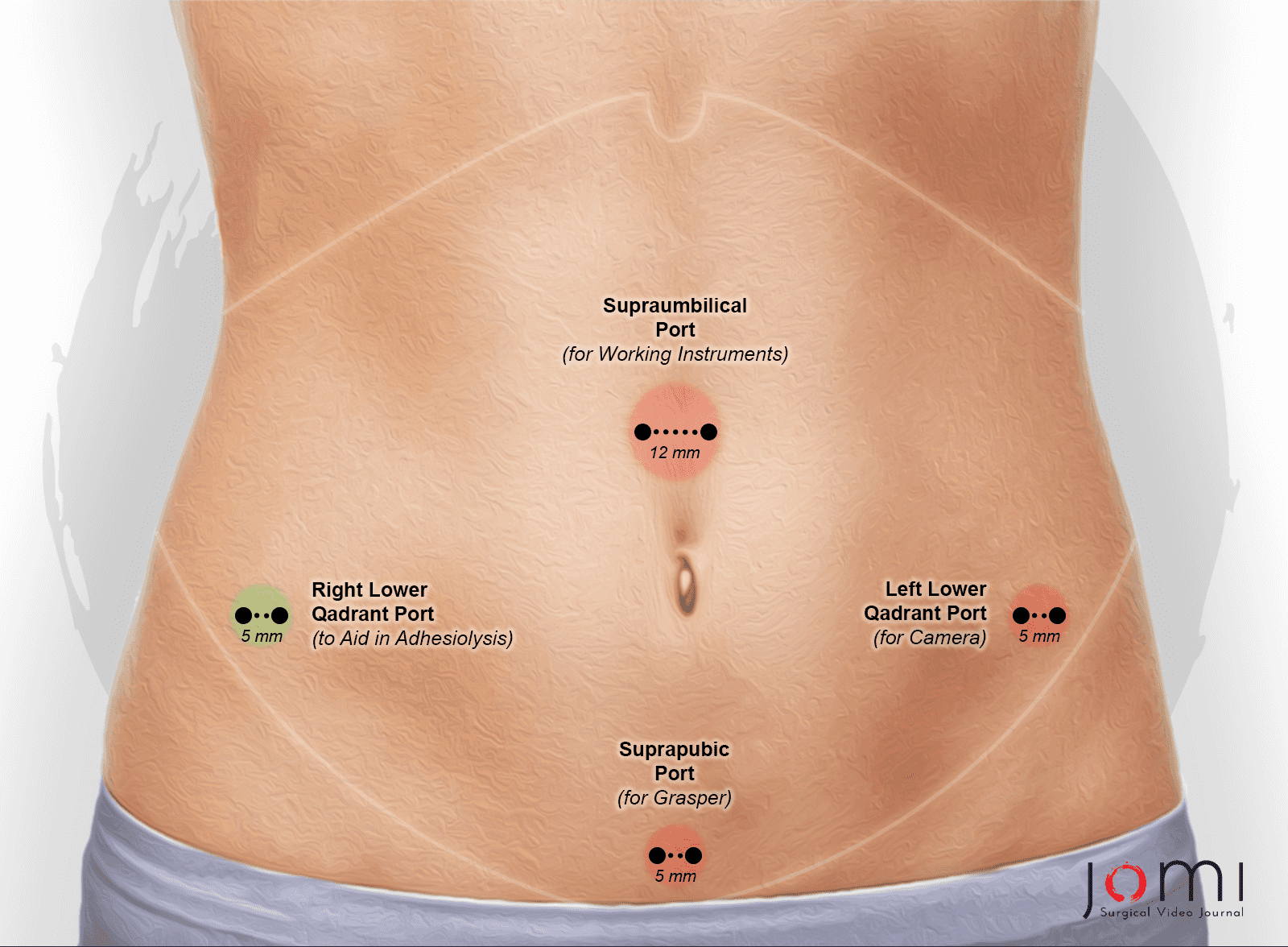
Figure 1. Port placement sites for laparoscopic appendectomy in a patient with prior umbilical hernia repair.
Following the lysis of adhesions, attention is turned to locating and exposing the appendix. The cecum is identified, and the appendix is carefully mobilized. In this case, the appendix is described as appearing inflamed and purple. The base of the appendix is noted to be relatively healthy in appearance. Once the appendix is adequately exposed, the mesoappendix is divided. This is accomplished using a bipolar sealing energy device. It is important that the appendiceal artery within the mesoappendix be meticulously identified and ligated to ensure adequate hemostasis during the procedure.
With the mesentery divided, the base of the appendix is carefully isolated. A 45-mm endoscopic stapler is used to divide and seal the base of the appendix. The stapler is carefully positioned to ensure complete resection of the appendix while preserving the integrity of the cecum.
After resection, the appendix is placed into a specimen retrieval bag system for removal from the abdominal cavity. The staple line is then inspected for hemostasis. Additional clips are applied to the staple line as a precautionary measure. The operative field is thoroughly irrigated and suctioned to remove any debris or contamination.
The procedure concludes with the closure of the port sites. The fascia at the larger port sites is closed using a figure-of-eight suture to prevent hernia formation. The skin is then approximated using subcuticular sutures and sealed with topical skin adhesive.
Throughout the procedure, careful attention is paid to maintaining proper visualization, ensuring hemostasis, and minimizing tissue trauma. Postoperatively, patients are advised to avoid lifting more than 10 pounds for approximately six weeks. Submerging the incisions underwater (e.g., bath, swimming) is discouraged for about one month to prevent infection. Patients are also informed about the importance of following up on the pathology results, as there is a rare possibility of incidental malignancy in appendix specimens.
This LA video serves as an educational tool, offering unique insights into complex surgical scenarios. It demonstrates real-time decision-making in the face of adhesions from previous surgery, showcasing how to adapt standard techniques to challenging anatomy. The video provides a clear visualization of advanced laparoscopic skills, including safe adhesiolysis, cautious dissection, and proper use of surgical devices. It emphasizes critical aspects of surgical safety, team communication, and complication management.
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Note
Animation added post-publication on 07/13/2025. No changes were made to the article content.
Abstract added post-publication on 07/21/2025 to meet indexing and accessibility requirements. No changes were made to the article content.
Citations
- Bessoff KE, Choi J, Wolff CJ, et al. Evidence-based surgery for laparoscopic appendectomy: a stepwise systematic review. Surg Open Sci. 2021;6. doi:10.1016/j.sopen.2021.08.001.
- Eltaweel MM. Laparoscopic versus open surgery for suspected appendicitis. Egypt J Hosp Med. 2022;88(1). doi:10.21608/ejhm.2022.246924.
- Biondi A, Di Stefano C, Ferrara F, Bellia A, Vacante M, Piazza L. Laparoscopic versus open appendectomy: a retrospective cohort study assessing outcomes and cost-effectiveness. World J Emerg Surg. 2016;11(1). doi:10.1186/s13017-016-0102-5.
- Moris D, Chakedis J, Rahnemai-Azar AA, et al. Postoperative abdominal adhesions: clinical significance and advances in prevention and management. J Gastrointest Surg. 2017;21(10). doi:10.1007/s11605-017-3488-9.
- Hassanabad AF, Zarzycki AN, Jeon K, Deniset JF, Fedak PWM. Post-operative adhesions: a comprehensive review of mechanisms. Biomedicines. 2021;9(8). doi:10.3390/biomedicines9080867.
- Szomstein S, Lo Menzo E, Simpfendorfer C, Zundel N, Rosenthal RJ. Laparoscopic lysis of adhesions. World J Surg. 2006;30(4). doi:10.1007/s00268-005-7778-0.

| Publication Date | 11/29/2024 |
| Article ID | 481 |
| Production ID | 0481 |
| Volume | 2024 |
| Issue | 481 |
| DOI | |
| https://doi.org/10.24296/jomi/481 | |